


Chikungunya in Latin America (2020–2025): Epidemiological Burden, Clinical Impact, and Public Health Priorities

Rosali Santiago Roibal  1; Deborah Cabrera Rodríguez 2; Lhianella Ramos Escobedo 2;Marlon Carbonell González 2*
1; Deborah Cabrera Rodríguez 2; Lhianella Ramos Escobedo 2;Marlon Carbonell González 2*
1All Behavior Community Inc., Florida, United States
2 High Quality Medical Services, Houston, United States.
*Corresponding author: Marlon Carbonell González: marloncarbonell95@gmail.com;
Tel: +1 (908) 926 1154..
ABSTRACT
Chikungunya virus (CHIKV) has maintained sustained transmission in Latin America since its introduction in 2013, generating recurrent outbreaks and a significant clinical, social, and economic burden. Between 2020 and 2025, more than 2.8 million suspected cases were reported, with Brazil contributing the highest morbidity and disability-adjusted life years (DALYs). Acute infection is characterized by sudden-onset fever, severe polyarthralgia, myalgia, headache, and a maculopapular rash. Approximately 40% of patients develop chronic arthropathy, which may persist for months or years, affecting functional capacity and quality of life. The diagnostic accuracy is challenged by the co-circulation of dengue and Zika, necessitating combined molecular and serological approaches. Management remains primarily supportive, utilizing NSAIDs, corticosteroids, and, in select cases, disease-modifying antirheumatic drugs (DMARDs) to manage persistent inflammation.
Transmission dynamics are driven by climatic variability, rapid urbanization, high densities of Aedes aegypti and Aedes albopictus, and increased human mobility. Considerable disparities exist in public health capacity across the region: Brazil has implemented robust surveillance and vector control, while Nicaragua, Bolivia, and parts of Peru face substantial limitations that delay outbreak detection and response. Although the Ixchiq vaccine was recently approved in high-income settings, access remains extremely limited in Latin American countries with endemic regions.
Strengthening genomic surveillance, integrating vector control with urban development policies, expanding equitable access to vaccination, and improving long-term care for chronic post-CHIKV sequelae are essential priorities. Future efforts should focus on genotype-specific transmission modeling, evaluating vaccine effectiveness in endemic populations, and coordinating cross-border data sharing to enhance early outbreak detection and regional preparedness.
Keywords: Chikungunya virus; Latin America; arboviruses; Aedes aegypti; Aedes albopictus; epidemiology; chronic arthropathy; public health; vector-borne diseases; surveillance.
INTRODUCTION
Chikungunya virus (CHIKV) is a mosquito-borne alphavirus primarily transmitted by Aedes aegypti and Aedes albopictus, both of which are prevalent in tropical and subtropical regions. 1 First identified in Tanzania in 1952, CHIKV has become a global public health concern due to its rapid geographic expansion, including the Americas, Asia, and parts of Europe. 2, 3 Introduced to the Americas in 2013, it has caused widespread epidemics, particularly in Latin America, affecting millions of people and overwhelming healthcare systems, as shown in Figure 1. 4
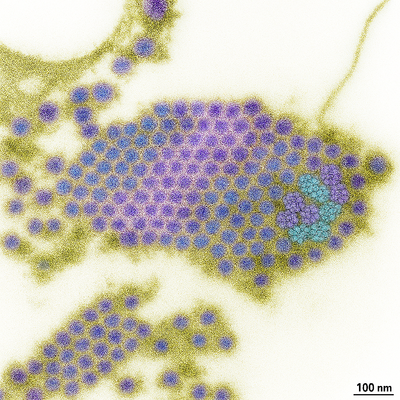
Figure 1. Chikungunya virus particles observed under high-resolution electron microscopy. High-resolution scanning electron micrograph illustrating multiple Chikungunya virus (CHIKV) particles. Each virion exhibits its characteristic spherical morphology, with a dense central nucleocapsid surrounded by a lipid envelope that contains surface glycoprotein spikes involved in host-cell attachment and entry. This structural organization underlies viral infectivity and facilitates transmission by Aedes mosquitoes.Figure generated by the authors using a custom AI-assisted workflow and validated against current structural virology literature.
Environmental, social, and economic factors strongly influence the epidemiology of CHIKV in Latin America.
Tropical and subtropical climates favor the proliferation of Aedes mosquitoes, while rapid, unplanned urbanization creates abundant breeding sites in densely populated areas. Climate change amplifies this risk by altering temperature and rainfall patterns, expanding the geographic range of vectors, and facilitating outbreaks in previously unaffected regions. 5 Additionally, high human mobility facilitates the introduction of the virus into new urban and peri-urban areas. The combination of urbanization, climate change, and human mobility creates an ideal environment for sustained CHIKV transmission, as shown in Figure 2. 6, 7
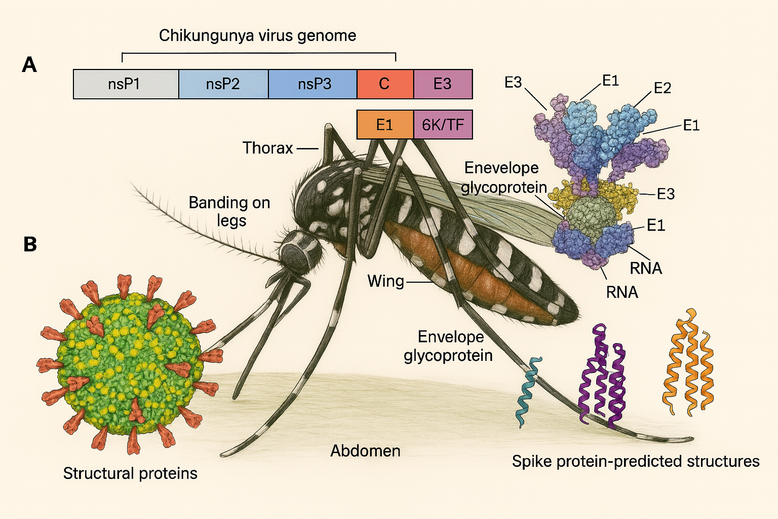
Figure 2. Genomic structure, virion architecture, and vector anatomy relevant to Chikungunya virus transmission.
Panel A: Schematic representation of the Chikungunya virus (CHIKV) genome, which encodes four nonstructural proteins (nsP1–nsP4) responsible for viral replication, and the structural proteins capsid (C), envelope glycoproteins (E1–E3), and 6K/TF, which are essential for virion assembly, budding, and host-cell entry.
Panel B: Structural depiction of the mature CHIKV virion showing its spherical morphology and the arrangement of envelope spike proteins composed of E1–E2–E3 glycoprotein complexes that mediate attachment and membrane fusion.
Central illustration: The Aedes mosquito vector highlighting diagnostic anatomical features—including thorax, abdomen, banding on legs, and wing structures—and the distribution of viral envelope glycoproteins associated with mosquito-mediated transmission. Predicted spike protein conformations involved in viral entry are shown at right.
Figure created by the authors using a custom AI-assisted workflow and validated against current genomic, structural, and entomological literature.
Panel A: Schematic representation of the Chikungunya virus (CHIKV) genome, which encodes four nonstructural proteins (nsP1–nsP4) responsible for viral replication, and the structural proteins capsid (C), envelope glycoproteins (E1–E3), and 6K/TF, which are essential for virion assembly, budding, and host-cell entry.
Panel B: Structural depiction of the mature CHIKV virion showing its spherical morphology and the arrangement of envelope spike proteins composed of E1–E2–E3 glycoprotein complexes that mediate attachment and membrane fusion.
Central illustration: The Aedes mosquito vector highlighting diagnostic anatomical features—including thorax, abdomen, banding on legs, and wing structures—and the distribution of viral envelope glycoproteins associated with mosquito-mediated transmission. Predicted spike protein conformations involved in viral entry are shown at right.
Figure created by the authors using a custom AI-assisted workflow and validated against current genomic, structural, and entomological literature.
Clinically, CHIKV infection manifests with sudden-onset fever, severe polyarthralgia, myalgia, headache, rash, and occasionally gastrointestinal or ocular symptoms. While most cases are self-limiting, many patients experience prolonged musculoskeletal symptoms, leading to functional impairment and reduced quality of life. 8, 9 Currently, no widely available specific antiviral therapy exists, and clinical management remains primarily supportive. 10 The recent approval of the Ixchiq vaccine represents a major advancement, although access in endemic Latin American regions remains limited, as shown in Figures 3 and 4. 11, 12, 13

Figure 3. Aedes albopictus is a competent vector of Chikungunya virus in tropical and subtropical regions.
High-resolution image of Aedes albopictus (the Asian tiger mosquito), a major vector of Chikungunya, Dengue, and Zika viruses. The species is characterized by distinctive black-and-white leg banding and a single white dorsal thoracic stripe. A. albopictus exhibits aggressive daytime biting behavior and high ecological adaptability, allowing it to thrive in both urban and peri-urban environments. Its expanding geographic range in the Americas has increased the risk of Chikungunya transmission, particularly in densely populated areas with favorable breeding sites.
Figure created by the authors using an AI-assisted image generation and refinement workflow and validated against entomological reference material.
Figure created by the authors using an AI-assisted image generation and refinement workflow and validated against entomological reference material.

Figure 4. Aedes aegypti is the principal urban vector of the Chikungunya virus in the Americas.
High-resolution image of Aedes aegypti, the primary urban vector for Chikungunya, Dengue, Zika, and yellow fever viruses. This species is identifiable by its lyre-shaped white dorsal markings on the thorax, banded legs, and its preference for feeding on humans (anthropophilic behavior). A. aegypti thrives in densely populated urban environments, breeds in artificial water containers, and exhibits peak biting activity during daylight hours. Its strong human–mosquito–human transmission cycle and high vector competence make it the dominant driver of Chikungunya outbreaks in Latin America.
Figure produced by the authors through an AI-assisted image generation and refinement workflow and validated using standard entomological references.
Figure produced by the authors through an AI-assisted image generation and refinement workflow and validated using standard entomological references.
CHIKV infection is associated with a broad spectrum of clinical manifestations, ranging from acute febrile illness to prolonged musculoskeletal symptoms. The pathogenesis involves viral entry, replication, and host immune responses, which together contribute to both acute and chronic disease phenotypes, as illustrated in
Figure 5. 14 Detailed mapping of pain and associated symptoms reveals distinct patterns in acute versus chronic CHIKV patients, highlighting common musculoskeletal and neurological manifestations and the prevalence of comorbidities, as shown in Figure 6. 9, 10
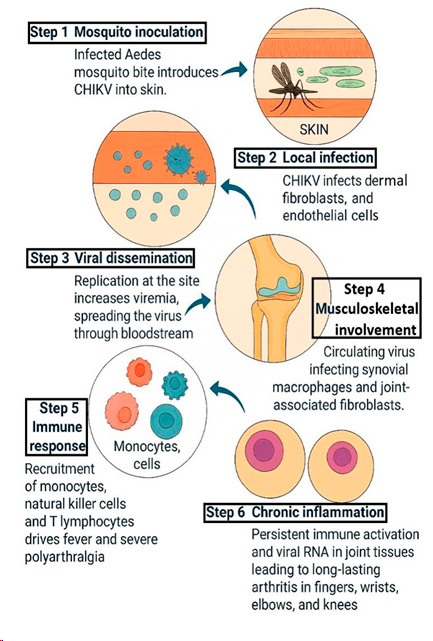
Figure 5. Pathogenesis of Chikungunya virus infection: from mosquito inoculation to systemic inflammation and joint involvement.
Schematic representation of the pathogenesis of Chikungunya virus (CHIKV) infection. Following inoculation of the virus into the skin by an infected Aedes mosquito (step 1), CHIKV initially infects dermal fibroblasts, macrophages, and endothelial cells (step 2). Viral replication at the inoculation site leads to increasing viremia and dissemination through the bloodstream (step 3). Circulating virus subsequently infects musculoskeletal tissues, including synovial macrophages and joint-associated fibroblasts (step 4), triggering a robust innate and adaptive immune response. Recruitment of inflammatory cells—such as monocytes, natural killer cells, and T lymphocytes—into infected tissues (step 5) contributes to the acute febrile phase and severe polyarthralgia. Persistent immune activation and viral RNA persistence in joint tissues may lead to chronic inflammation and long-lasting arthritis that can affect fingers, wrists, elbows, and knees (step 6).
Figure created by the authors using an AI-assisted illustration workflow and validated against current immunopathogenesis and clinical literature on CHIKV.
Figure created by the authors using an AI-assisted illustration workflow and validated against current immunopathogenesis and clinical literature on CHIKV.
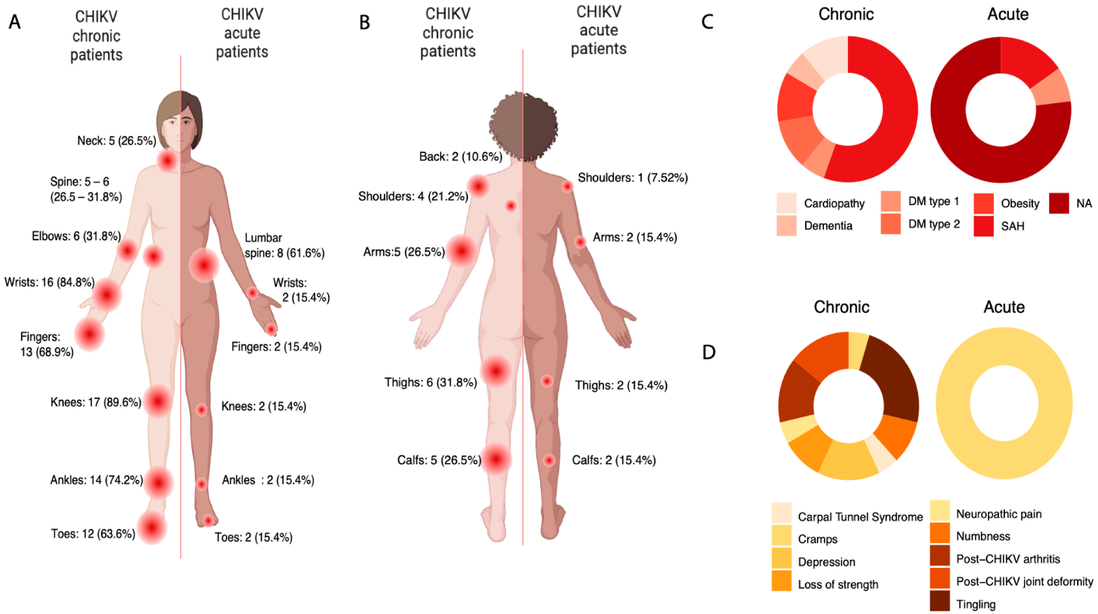
Figure 6. Anatomical distribution of pain, comorbidities, and symptom profiles in acute and chronic Chikungunya virus (CHIKV) infection.
Panel A: Anterior anatomical mapping of pain distribution in patients with chronic CHIKV infection (left) compared with acute-phase patients (right). Chronic cases exhibit a markedly higher frequency and wider distribution of joint involvement—particularly in the wrists, knees, ankles, fingers, and elbows—consistent with persistent post-CHIKV arthropathy.
Panel B: Posterior view illustrating musculoskeletal pain localization in chronic (left) and acute (right) patients. Chronic cases present greater involvement of the shoulders, arms, back, and thighs, reflecting the transition from acute inflammation to sustained musculoskeletal dysfunction.
Panel C: Comparative prevalence of comorbidities in chronic versus acute CHIKV cohorts, including obesity, diabetes mellitus types 1 and 2, systemic arterial hypertension (SAH), cardiopathy, and dementia. A higher comorbidity burden in chronic cases suggests an increased susceptibility to prolonged inflammation and delayed recovery.
Panel D: Symptom profiles highlighting distinctions between chronic and acute CHIKV presentations. Chronic patients more commonly exhibit neuropathic pain, carpal tunnel syndrome, cramps, depression, post-CHIKV arthritis, joint deformity, loss of strength, and persistent tingling, whereas acute cases primarily report transient systemic symptoms without long-term sequelae.
Visual data reflect patient-reported outcomes and standardized clinical assessments during post-CHIKV follow-up. Figure created using an AI-assisted illustration workflow and validated against current clinical and rheumatological literature on CHIKV sequelae.
Panel B: Posterior view illustrating musculoskeletal pain localization in chronic (left) and acute (right) patients. Chronic cases present greater involvement of the shoulders, arms, back, and thighs, reflecting the transition from acute inflammation to sustained musculoskeletal dysfunction.
Panel C: Comparative prevalence of comorbidities in chronic versus acute CHIKV cohorts, including obesity, diabetes mellitus types 1 and 2, systemic arterial hypertension (SAH), cardiopathy, and dementia. A higher comorbidity burden in chronic cases suggests an increased susceptibility to prolonged inflammation and delayed recovery.
Panel D: Symptom profiles highlighting distinctions between chronic and acute CHIKV presentations. Chronic patients more commonly exhibit neuropathic pain, carpal tunnel syndrome, cramps, depression, post-CHIKV arthritis, joint deformity, loss of strength, and persistent tingling, whereas acute cases primarily report transient systemic symptoms without long-term sequelae.
Visual data reflect patient-reported outcomes and standardized clinical assessments during post-CHIKV follow-up. Figure created using an AI-assisted illustration workflow and validated against current clinical and rheumatological literature on CHIKV sequelae.
Comparative analyses of mosquito-borne diseases reveal differences in symptom frequency and severity, which are crucial for differential diagnosis in endemic regions. Fever, rash, inflammatory arthritis, myalgia, and headache are among the most frequent clinical features, with variations in presentation between Dengue, Chikungunya, and Zika infections, summarized in Figure 7. 9, 10 Additionally, the typical cutaneous and arthritic manifestations observed in acute and chronic chikungunya infection, including maculopapular rash and periarticular swelling, are illustrated in Figure 8, highlighting the clinical patterns that may persist or resolve asymmetrically. Including these comparative symptom profiles and illustrative manifestations in the review provides a clearer understanding of CHIKV's clinical burden, supporting targeted public health interventions. 15, 16
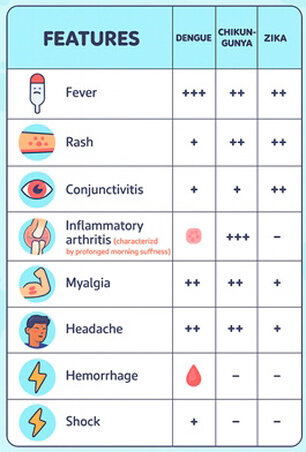
Figure 7. Comparative clinical features of Dengue, Chikungunya, and Zika virus infections.
Comparative chart summarizing the relative frequency and intensity of major clinical manifestations associated with Dengue, Chikungunya, and Zika virus infections. Fever and headache occur most prominently in Dengue, while rash and conjunctivitis are more characteristic of Zika. Chikungunya is distinguished by its hallmark inflammatory arthritis—often severe and prolonged, with morning stiffness—alongside frequent myalgia. Hemorrhagic manifestations and shock are predominantly associated with severe Dengue, reflecting its vascular permeability and plasma leakage pathophysiology. The symptom-based comparison assists clinicians in differential diagnosis in regions where these arboviruses co-circulate. Figure created using an AI-assisted illustration workflow and validated against current clinical and epidemiological literature on arboviral disease presentations.
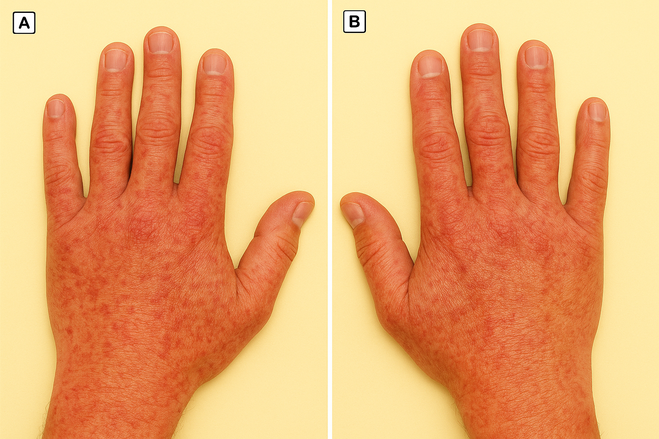
Figure 8. Cutaneous and periarticular manifestations during acute Chikungunya virus infection. Panel A: Dorsal view of the left hand showing an intense erythematous maculopapular rash accompanied by periarticular swelling, consistent with acute-phase Chikungunya virus (CHIKV) infection. The combination of diffuse rash and early inflammatory edema around the metacarpophalangeal and interphalangeal joints reflects the characteristic viral-induced synovitis and soft-tissue inflammation.
Panel B: Right hand demonstrating similar dermatologic findings but with reduced erythema and swelling, suggesting partial clinical improvement or asymmetric involvement—both recognized patterns in CHIKV-associated arthropathy.
These dermatologic and articular manifestations are typical of the acute phase of CHIKV infection, where rash often resolves within days and may be followed by transient desquamation. Persistent joint discomfort may evolve into chronic post-CHIKV arthritis in a subset of patients.
Figure produced using an AI-assisted medical illustration workflow and validated against current dermatological and rheumatological literature on Chikungunya virus infection.
Panel B: Right hand demonstrating similar dermatologic findings but with reduced erythema and swelling, suggesting partial clinical improvement or asymmetric involvement—both recognized patterns in CHIKV-associated arthropathy.
These dermatologic and articular manifestations are typical of the acute phase of CHIKV infection, where rash often resolves within days and may be followed by transient desquamation. Persistent joint discomfort may evolve into chronic post-CHIKV arthritis in a subset of patients.
Figure produced using an AI-assisted medical illustration workflow and validated against current dermatological and rheumatological literature on Chikungunya virus infection.
In summary, CHIKV transmission in Latin America results from a complex interplay among viral biology, vector ecology, environmental factors, urbanization, and social determinants. This narrative review aims to synthesize recent evidence on chikungunya infection, its clinical consequences, and public health responses in the region, with a comprehensive focus encompassing both clinical care and prevention and control strategies.
Clinical and Epidemiological Overview of Chikungunya in Latin America
Epidemiology
Since its introduction in the Americas in 2013, CHIKV has demonstrated persistent endemicity and recurrent outbreaks across Latin America. Between 2020 and 2025, Brazil continued to be the epicenter of CHIKV activity, reporting over 1.7 million suspected cases, with substantial outbreaks in northeastern and southeastern regions. Colombia, Nicaragua, Bolivia, and Peru also experienced significant CHIKV activity, with peaks corresponding to seasonal rainfall and higher vector density. 17, 18, 19 Regional surveillance data indicate that CHIKV outbreaks are often cyclical, with intervals of low transmission followed by explosive epidemic events, a pattern influenced by climate variability, vector population dynamics, and human mobility. Recent studies estimate that CHIKV contributes >1 million DALYs annually in Latin America, reflecting both acute morbidity and long-term disability from chronic arthropathy. 20, 21 These data are summarized in Table 1.
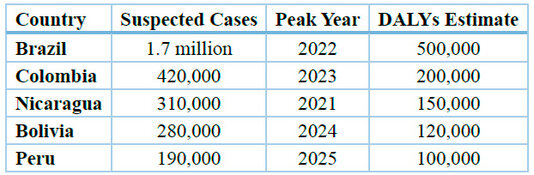
Table 1. Epidemiological burden of CHIKV in major Latin American countries (2020–2025).
Data compiled from national surveillance systems and regional estimates from CDC¹, PAHO4,16, and WHO8,14. DALY approximations based on regional burden assessments reported in Lancet Reg Health Am3 and Trans R Soc Trop Med Hyg10,11.
Clinical Features
CHIKV infection typically presents with sudden-onset high fever, severe polyarthralgia, myalgia, headache, and a maculopapular rash. 22 Gastrointestinal symptoms, including nausea, vomiting, and diarrhea, occur in a subset of patients, while ocular manifestations, such as conjunctivitis, have also been reported. 23 Notably, chronic post-viral arthropathy affects up to 40% of patients, persisting for months or even years and contributing to functional impairment, decreased quality of life, and economic loss due to reduced productivity. 24 Comorbidities such as diabetes, hypertension, and pre-existing joint disease are associated with increased severity of CHIKV-related arthropathy and prolonged recovery. Recent cohort studies indicate that older adults and individuals with immunocompromising conditions are at higher risk for severe manifestations, including neurological complications and protracted fatigue. 25, 26 Table 2 presents these findings.
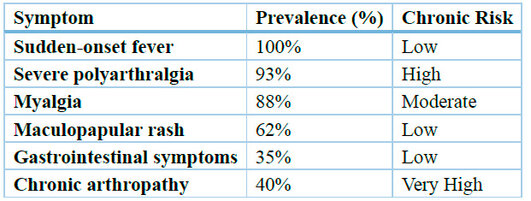
Note: Chronic arthropathy may persist for months to years, particularly in older adults or in patients with diabetes, hypertension, or pre-existing joint disorders.
Table 2. Clinical features and chronic sequelae associated with Chikungunya virus (CHIKV) infection. Clinical frequency and long-term sequelae of CHIKV infection, based on regional cohort studies and global clinical summaries from WHO8⁽²⁰²⁵⁾, PAHO4,16, and recent longitudinal analyses addressing post-CHIKV musculoskeletal disability (Lancet Reg Health Am3; Trans R Soc Trop Med Hyg10,11). Severe polyarthralgia is the hallmark of acute infection and is strongly associated with the development of chronic post-viral arthropathy, which accounts for a substantial portion of the estimated DALY burden in affected populations.
Diagnosis
Laboratory confirmation of CHIKV infection relies on RT-PCR during the acute phase (the first 5–7 days of illness), which offers high sensitivity and specificity. 27 In the subacute phase, IgM serology is commonly used; IgG seroconversion indicates past exposure. Typical laboratory findings include leukopenia, thrombocytopenia, mild transaminase elevations, and, occasionally, elevated inflammatory markers, such as CRP and ESR. 28, 29 Diagnostic accuracy is influenced by the timing of sample collection, viral load, and co-circulation of other arboviruses such as Dengue and Zika, which can lead to cross-reactivity and misdiagnosis if serological testing is used in isolation. Recent studies recommend combining molecular and serological assays to improve diagnostic reliability in endemic regions. 30, 31
Management
There is currently no specific antiviral therapy for CHIKV infection. 32 Management is primarily supportive, focusing on hydration, rest, and analgesia. 33 NSAIDs are widely used to alleviate arthralgia and myalgia, while corticosteroids may be indicated in severe inflammatory cases or in patients with debilitating chronic arthritis. Antipyretic agents, including paracetamol, are recommended for the management of fever. 34, 35 Recent clinical reports have explored adjunctive therapies, such as disease-modifying antirheumatic drugs (DMARDs), for persistent post-CHIKV arthropathy, though evidence remains limited. Early supportive care has been associated with shorter disease duration, reduced symptom severity, and improved functional outcomes. 36, 37
Public Health Strategies
Vector control remains the cornerstone of CHIKV prevention. Integrated vector management strategies include eliminating mosquito breeding sites, implementing larvicidal and adulticidal interventions, deploying insecticide-treated materials, and conducting public education campaigns. 38, 39 Surveillance systems in Brazil, Colombia, and other Latin American countries have been enhanced with real-time reporting, geographic mapping of cases, and predictive modeling to identify and anticipate outbreak hotspots. 40 The recent approval of the CHIKV vaccine Ixchiq in Europe and the United States represents a milestone in preventive strategies; however, its deployment in endemic Latin American regions remains limited. 41 Comparative analyses of outbreaks from 2020 to 2025 indicate that countries with robust vector control, early case detection, and community engagement experience shorter outbreak durations, lower morbidity, and reduced economic impact. 42 Table 3 summarizes these data.
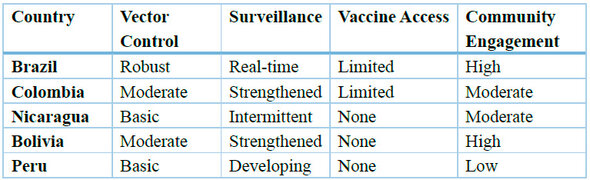
Table 3. Public Health Strategies for Chikungunya Virus (CHIKV) Control in Selected Latin American Countries (2020–2025). Comparative overview of national public health strategies for CHIKV control in Latin America between 2020 and 2025.
Data compiled from national epidemiological bulletins, WHO regional updates8,14, PAHO situation reports4,16, and publicly available regulatory information on chikungunya vaccine availability (Valneva/FDA/EMA reports5,13,20). Vaccine deployment remains limited across endemic regions, with no large-scale public immunization campaigns implemented. Countries that combine robust vector control, enhanced surveillance (including genomic monitoring), and sustained community participation—such as Brazil—tend to experience shorter outbreak durations and lower morbidity.
Clinical Insights and Public Health Implications
Chikungunya virus (CHIKV) remains a major public health concern in Latin America. Since its introduction to the Americas in 2013, recurrent outbreaks have demonstrated the complexity of controlling vector-borne diseases in densely populated urban settings. Factors such as climate change, rapid urbanization, and increased human mobility have facilitated the spread of viruses, compounding the challenges faced by public health authorities. Recent analyses confirm that localized urban factors, such as housing quality and population density, are more critical for predicting outbreak magnitude than climate alone. 43, 44, 45
Epidemiology and Distribution
Brazil has consistently been the epicenter of CHIKV activity in Latin America, reporting over 1.7 million suspected cases between 2017 and 2024. This is consistent with the most recent data, which places Brazil as the Americas' highest-case burden, accounting for 96% of the region's confirmed cases and deaths as of August 2025. 46, 47. Other countries, including Colombia, Nicaragua, Bolivia, and Peru, have also experienced substantial outbreaks, often peaking during rainy seasons and periods of increased vector density. Regional surveillance data indicate that CHIKV outbreaks follow a cyclical pattern, with periods of low transmission interrupted by explosive epidemics influenced by climatic variability, vector population dynamics, and human movement. A concerning shift noted by PAHO is the co-circulation of the East/Central/South African (ECSA) genotype alongside the Asian genotype in at least four countries, which could enhance viral adaptation and transmission dynamics. 48
For instance, Brazil has implemented robust surveillance systems with real-time reporting and genomic monitoring, enabling earlier detection of outbreaks and more coordinated public health responses. In contrast, Nicaragua has faced recurrent epidemics with limited diagnostic capacity and fewer resources for sustained vector control, resulting in delayed recognition of outbreaks and higher community-level transmission. This contrast highlights how differences in health system infrastructure and resource allocation directly influence the scale and duration of CHIKV epidemics in Latin America. 49, 50
Clinical Features and Disease Burden
CHIKV infection typically manifests with sudden-onset high fever, severe polyarthralgia, myalgia, headache, and a maculopapular rash. Gastrointestinal symptoms (nausea, vomiting, diarrhea) and ocular manifestations (conjunctivitis) have been reported in a subset of patients. While most infections are self-limited, chronic post-viral arthropathy affects up to 40% of patients, persisting for months or years and causing significant functional impairment, decreased quality of life, and economic losses due to reduced productivity. Recent authors strongly support this burden, documenting that chronic joint pain affects a significant proportion of patients and can lead to long-term disability and socioeconomic burden. Comorbidities such as diabetes, hypertension, and pre-existing joint disorders increase the risk of severe arthropathy and prolonged recovery. Older adults and immunocompromised individuals are particularly susceptible to severe manifestations, including neurological complications and chronic fatigue. 30
Diagnosis and Clinical Management
Laboratory confirmation relies on RT-PCR during the acute phase (first 5–7 days) and IgM serology in the subacute phase, with IgG indicating prior exposure. Laboratory abnormalities often include leukopenia, thrombocytopenia, mild elevation of liver enzymes, and occasionally elevated inflammatory markers such as CRP and ESR. Diagnostic accuracy can be affected by sample timing, viral load, and the presence of co-circulating arboviruses (e.g., Dengue, Zika), which can lead to serological cross-reactivity. Combining molecular and serological assays is recommended to improve diagnostic reliability in endemic regions.
Currently, there is no specific antiviral treatment for CHIKV infection. Management is primarily supportive, including hydration, rest, and analgesics. Non-steroidal anti-inflammatory drugs (NSAIDs) are widely used to alleviate arthralgia and myalgia, while corticosteroids may be indicated in severe inflammatory cases or debilitating chronic arthritis. Antipyretics, such as paracetamol, are recommended for controlling fever. This management approach is consistently endorsed by recent systematic reviews, which confirm the lack of a specific antiviral treatment and the need for a symptomatic approach. 35 Recent studies have explored adjunctive therapies, including disease-modifying antirheumatic drugs (DMARDs) for persistent post-CHIKV arthropathy, although evidence remains limited.
To our knowledge, this review represents one of the most recent and regionally focused syntheses (2020–2025) examining the epidemiological burden, clinical impact, diagnostic challenges, and public health strategies related to Chikungunya in Latin America.
By integrating epidemiological data, clinical evidence, and policy insights, this narrative review aims to clarify evolving transmission patterns, highlight persistent gaps in regional preparedness, and identify priority actions to reduce the long-term impact of CHIKV on public health systems in the Americas.
By integrating epidemiological data, clinical evidence, and policy insights, this narrative review aims to clarify evolving transmission patterns, highlight persistent gaps in regional preparedness, and identify priority actions to reduce the long-term impact of CHIKV on public health systems in the Americas.
CONCLUSIONS
Effective control of CHIKV in Latin America requires a coordinated approach that addresses clinical, public health, and research priorities. Clinically, CHIKV continues to pose challenges: sudden-onset fever, severe polyarthralgia, and chronic post-viral arthropathy affect a substantial proportion of patients, particularly older adults and those with comorbidities, leading to functional impairment and socioeconomic burden. Supportive care—including hydration, analgesics, NSAIDs, corticosteroids for severe inflammatory cases, and DMARDs for persistent arthropathy—remains essential, alongside timely diagnosis in regions with co-circulating arboviruses.
At the public health level, integrated vector control, robust surveillance, and equitable vaccine distribution are critical. Countries like Brazil, with real-time reporting, genomic monitoring, and predictive modeling, have achieved more effective outbreak containment, whereas resource-limited settings, such as Nicaragua, face delayed detection and higher transmission. The deployment of the recently approved Ixchiq vaccine offers a promising preventive tool; however, equitable access across low- and middle-income countries will require regional coordination, joint procurement, and community engagement. Genotype co-circulation (ECSA and Asian) and the evolution of urban and environmental risk factors underscore the need for adaptive, context-specific strategies.
From a research perspective, developing next-generation vaccines and antiviral therapies, understanding genotype-specific transmission dynamics, and climate-linked epidemiological modeling are crucial for guiding targeted interventions. Strengthening surveillance networks, integrating genomic sequencing and vector monitoring, and promoting cross-border data sharing will enhance early outbreak detection and response capacity.
By combining clinical vigilance, integrated vector management, equitable vaccination, and research-informed strategies, Latin America can advance sustainable chikungunya control and reduce the burden of future outbreaks.
Author Contributions: Conceptualization, Rosali Santiago Roibal (R.S.R.), Marlon Carbonell González (M.C.G.) and Deborah Cabrera Rodríguez (D.C.R.); methodology, M.C.G.; validation, M.C.G., R.S.R. and Lhianella Ramos Escobedo (L.R.E.); formal analysis, M.C.G.; investigation, M.C.G. and D.C.R.; resources, R.S.R.; data curation, L.R.E.; writing—original draft preparation, M.C.G.; writing—review and editing, R.S.R., D.C.R. and L.R.E.; visualization, M.C.G.; supervision, R.S.R.; project administration, M.C.G.; funding acquisition, none.
All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
The Article Processing Charge (APC) was self-funded by the corresponding author.
Institutional Review Board Statement: Not applicable.
This study did not involve humans or animals and was conducted entirely through the review and synthesis of published literature in accordance with the Declaration of Helsinki.
Informed Consent Statement: Not applicable.
This article is a literature-based review and did not involve human participants or identifiable data.
Data Availability Statement: No new data were created or analyzed in this study.
Data sharing is therefore not applicable.
All data supporting the findings of this study are available in the references cited.
Data sharing is therefore not applicable.
All data supporting the findings of this study are available in the references cited.
Acknowledgments: The authors express their gratitude to the staff of the Intensive Care Unit at Miguel Enríquez Faculty of Medical Sciences and the Department of Epidemiology at the University of Medical Sciences of Matanzas for their invaluable support and guidance during data collection and review. We also thank regional public health authorities for providing epidemiological data and facilitating access to surveillance databases, which were essential for the successful completion of this study.
Conflicts of Interest: The authors declare no conflict of interest.
The authors alone are responsible for the content and writing of this paper.
The authors alone are responsible for the content and writing of this paper.
Data and AI Disclosure:
All figures and tables were created by the authors using publicly available data and the scientific resources cited in this manuscript. Figures 1–8 were generated using author-supervised AI-assisted illustration workflows (OpenAI Copilot) based exclusively on established scientific knowledge; no AI tool generated new data or scientific interpretations. Generative artificial intelligence was used solely for linguistic editing, grammatical correction, and formatting standardization, always under full human supervision. No AI system was used for data generation, data analysis, or the creation of original scientific content. The authors independently verified all scientific information, interpretations, and conclusions in accordance with BioNatura Journal's policy on AI-assisted content (https://bionaturajournal.com/artificial-intelligence--ai-.html).
All figures and tables were created by the authors using publicly available data and the scientific resources cited in this manuscript. Figures 1–8 were generated using author-supervised AI-assisted illustration workflows (OpenAI Copilot) based exclusively on established scientific knowledge; no AI tool generated new data or scientific interpretations. Generative artificial intelligence was used solely for linguistic editing, grammatical correction, and formatting standardization, always under full human supervision. No AI system was used for data generation, data analysis, or the creation of original scientific content. The authors independently verified all scientific information, interpretations, and conclusions in accordance with BioNatura Journal's policy on AI-assisted content (https://bionaturajournal.com/artificial-intelligence--ai-.html).
REFERENCES
1. Centers for Disease Control and Prevention. Chikungunya in the United States. 2025 [cited 2025 Oct 24]. Available from: https://www.cdc.gov/chikungunya/data-maps/chikungunya-us.html
2. World Health Organization. Chikungunya fact sheet. April 14, 2025 [cited 2025 Oct 24]. Available from: https://www.who.int/news-room/fact-sheets/detail/chikungunya
3. de Souza WM, de Lima STS, Simões Mello LM, Candido DS, Buss L, Whittaker C, Claro IM, Chandradeva N, Granja F, de Jesus R, Lemos PS, Toledo-Teixeira DA, Barbosa PP, Firmino ACL, Amorim MR, Duarte LMF, Pessoa IB Jr, Forato J, Vasconcelos IL, Maximo ACBM, Araújo ELL, Perdigão Mello L, Sabino EC, Proença-Módena JL, Faria NR, Weaver SC. Spatiotemporal dynamics and recurrence of chikungunya virus in Brazil: an epidemiological study. Lancet Microbe. 2023 May;4(5):e319-e329. Available from: https://doi.org/10.1016/S2666-5247(23)00033-2.
4. Pan American Health Organization. Amid localized chikungunya outbreaks and ongoing Oropouche cases, PAHO urges strengthened surveillance and vector control across the Americas. 2025 [cited 2025 Oct 24]. Available from: https://www.paho.org/en/news/29-8-2025-amid-localized-chikungunya-outbreaks-and-ongoing-oropouche-cases-paho-urges
5. European Medicines Agency. CHMP recommends suspension of chikungunya vaccine in elderly population. EMA; 2025 [cited 2025 Oct 24]. Available from: https://www.ema.europa.eu/en/news/chmp-recommends-suspension-chikungunya-vaccine-elderly
6. U.S. Centers for Disease Control and Prevention. CDC Advisory Committee on Immunization Practices (ACIP) recommendations for chikungunya vaccine. CDC; 2025 [cited 2025 Oct 24]. Available from: https://www.cdc.gov/vaccines/acip/chikungunya
7. Medicines and Healthcare products Regulatory Agency (MHRA). MHRA suspends authorization of chikungunya vaccine in elderly adults. UK MHRA; 2025 [cited 2025 Oct 24]. Available from: https://www.gov.uk/drug-safety-update/chikungunya-vaccine-suspension
8. World Health Organization. Chikungunya fact sheet. 2025 [cited 2025 Oct 24]. Available from: https://www.who.int/news-room/fact-sheets/detail/chikungunya
9. Cerqueira-Silva T, Cardim LL, Paixão E, Rossi M, Santos AC, Portela F de Souza A, Santos G, Barreto ML, Brickley EB, Pescarini JM. Hospitalisation, mortality and years of life lost among chikungunya and dengue cases in Brazil: a nationwide cohort study, 2015-2024. Lancet Reg Health Am. 2025 Jul 7;49:101177. Available from: https://doi.org/10.1016/j.lana.2025.101177
10. de Roo AM, Vondeling GT, Boer M, Murray K, Postma MJ. The global health and economic burden of chikungunya from 2011 to 2020: a model-driven analysis on the impact of an emerging vector-borne disease. BMJ Glob Health. 2024 Dec 3;9(12):e016648. Available from: https://doi.org/10.1136/bmjgh-2024-016648
11. Tiozzo G, de Roo AM, Gurgel do Amaral GS, Hofstra H, Vondeling GT, Postma MJ. Assessing chikungunya's economic burden and impact on health-related quality of life: Two systematic literature reviews. PLoS Negl Trop Dis. 2025 May 5;19(5):e0012990. Available from: https://doi.otg/10.1371/journal.pntd.0012990
12. Li Z, Li Y, Li C. Re-emergence of chikungunya virus in China by 2025. PLoS Pathog. 2025;21(10):e1013556. Available from: https://doi.org/10.1371/journal.ppat.1013556
13. European Medicines Agency. First chikungunya vaccine recommended for approval in the European Union. EMA; 2025 [cited 2025 Oct 24]. Available from: https://www.ema.europa.eu/en/news/first-chikungunya-vaccine-recommended-approval-eu
14. World Health Organization. Chikungunya epidemiology update – June 2025. 2025 [cited 2025 Oct 24]. Available from: https://www.who.int/publications/m/item/chikungunya-epidemiology-update-june-2025
15. Wang L, Zheng Y, Wang K. Estimating the transmissibility of the 2025 chikungunya fever outbreak in Foshan, China: a modelling study. Infect Dis Poverty. 2025;14:106. Available from: https://doi.org/10.1186/s40249-025-01376-8
16. Pan American Health Organization. Chikungunya. 2024 [cited 2025 Oct 24]. Available from: https://www.paho.org/es/temas/chikungunya
17. Ribeiro Dos Santos G, Jawed F, Mukandavire C, Deol A, Scarponi D, Mboera LEG, Seruyange E, Poirier MJP, Bosomprah S, Udeze AO, Dellagi K, Hozé N, Chilongola J, Nasrallah GK, Cauchemez S, Salje H. Global burden of chikungunya virus infections and the potential benefit of vaccination campaigns. Nat Med. 2025 Jul;31(7):2342-2349. Available from: https://doi.org/10.1038/s41591-025-04065-z
18. Centers for Disease Control and Prevention. Transmisión del virus del chikunguña. 2024 [cited 2025 Oct 24]. Available from: https://www.cdc.gov/chikungunya/es/php/transmission/transmision-del-virus-del-chikunguna.html
19. World Health Organization. Chikungunya virus disease – Global situation. Disease Outbreak News. 2025 [cited 2025 Oct 24]. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2025-DON581
20. U.S. Food and Drug Administration. FDA approves first chikungunya vaccine. FDA; 2025 [cited 2025 Oct 24]. Available from: https://www.fda.gov/vaccines-blood-biologics/chikungunya-vaccine-approval
21. Volkova E, Langevin E, Lorenzo M, et al. Safety and immunogenicity of a single-shot live-attenuated chikungunya vaccine: a double-blind, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2023;401(10394):2138-2147. Available from: https://doi.org/10.1016/S0140-6736(23)00641-4
22. Centers for Disease Control and Prevention (CDC). Notes from the Field: Chikungunya Outbreak - Paraguay, 2022-2023. MMWR Morb Mortal Wkly Rep. 2023;72(23):636-638. Available from: https://doi.org/10.15585/mmwr.mm7223a5
23. Galan-Huerta KA, Rivas-Estilla AM, Fernández-Salas I, Farfan-Ale JA, Ramos-Jimenez J. Chikungunya virus: A general overview. Medicina Universitaria. 2025. Available from: https://doi.org/10.1016/j.rmu.2025.100150
24. Burden of Chikungunya Fever and Its Economic and Social Impacts Worldwide: A Systematic Review. Trop Med Int Health. 2025;30(9):865-892. Available from: https://doi.org/10.1111/tmi.70012
25. Public Health Agency of Canada, BCCDC Public Health Laboratory, Alberta Precision Laboratories, Public Health Ontario Laboratory. Travel-related dengue, Zika and chikungunya in Canada, 2024: Update to results from a feasibility pilot study on laboratory-based surveillance. Can Commun Dis Rep. 2025;51(9):374. Available from: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2025-51/issue-9-september-2025/travel-related-dengue-zika-chikungunya-canada-2024.html
26. Staples JE, Hills SL, Powers AM. Chikungunya. In: CDC Yellow Book 2026: Health Information for International Travel. Centers for Disease Control and Prevention; 2025. Accessed August 26, 2025. Available from: https://www.cdc.gov/yellow-book/hcp/travel-associated-infections-diseases/chikungunya.html
27. Feng Y, Chang F, Yang Y, et al. From dengue to chikungunya: Guangdong as a sentinel for arboviral threats in East Asia. Biosci Trends. 2025;19:368-373. Available from: https://doi.org/10.5582/bst.2025.01228
28. Li Y, Jiang S, Zhang M, et al. An outbreak of Chikungunya fever in China - Foshan City, Guangdong Province, China, July 2025. China CDC Wkly. 2025;7:1064-1065. Available from: https://doi.org/10.46234/ccdcw2025.172
29. Chikungunya fever: pathogenesis and mechanisms underlying pain symptoms. Front Immunol. 2025;16. Available from: https://doi.org/10.3389/fimmu.2025.1679385
30. Current landscape with an analytical outlook: Chikungunya virus vaccine development. The Innovation Med. 2025:100173. Available from: https://doi.org/10.59717/j.xinn-med.2025.100173
31. Kang H, Auzenbergs M, Clapham H, et al. Chikungunya seroprevalence, force of infection, and prevalence of chronic disability after infection in endemic and epidemic settings: A systematic review, meta-analysis, and modelling study. Lancet Infect Dis. 2024;24(5):488-503. Available from: https://doi.org/10.1016/S1473-3099(23)00810-1
32. de Souza WM, de Lima STS, Simoes Mello LM, et al. Spatiotemporal dynamics and recurrence of chikungunya virus in Brazil: An epidemiological study. Lancet Microbe. 2023;4(5):e319-e329. Available from: https://doi.org/10.1016/S2666-5247(23)00033-2
33. Tiozzo G, de Roo AM, Gurgel do Amaral GS, et al. Assessing chikungunya's economic burden and impact on health-related quality of life: Two systematic literature reviews. PLoS Negl Trop Dis. 2025;19(8):e0012990. Available from: https://doi.org/10.1371/journal.pntd.0012990
34. Bartholomeeusen K, Daniel M, Lassaus L, Mercer L, Hast M, Gasque P. Chikungunya fever. Nat Rev Dis Primers. 2023;9:17. Available from: https://doi.org/10.1038/s41572-023-00429-2
35. Mendoza-Roldan JA, Otranto D. Zoonotic arthropod-borne parasites in the Americas. Trends Parasitol. 2023;39(7):554-576. Available from: https://doi.org/10.1016/j.pt.2023.04.005
36. Pezzi L, Laureno M, Rezende IM, et al. Re-emergence of chikungunya in the Americas: An ongoing public health challenge. Viruses. 2023;15(8):1762. Available from: https://doi.org/10.3390/v15081762
37. Cavalcanti LPG, de Oliveira CDL, de Almeida MM, et al. The economic burden of the Chikungunya epidemic in Brazil: a cost-of-illness study, 2016-2019. Value Health Reg Issues. 2024;40:100-107. Available from: https://doi.org/10.1016/j.vhri.2024.01.008
38. Naveca FG, Nascimento VAD, Nascimento FMD, et al. Genomic and epidemiological of Chikungunya virus in the Brazilian Amazon region, 2014-2022. Viruses. 2024;16(4):542. Available from: https://doi.org/10.3390/v16040542
39. Cardona-Ospina JA, Henao-SanMartin V, Paniz-Mondolfi AE, Rodriguez-Morales AJ. The escalating burden of Chikungunya in Latin America: a call for integrated surveillance and control. Trop Med Infect Dis. 2024;9(3):65. Available from: https://doi.org/10.3390/tropicalmed9030065
40. Teixeira MG, da Conceição NMD, de Oliveira CDL, et al. Spatial and temporal dynamics of a major Chikungunya outbreak in a metropolitan area of Brazil, 2021-2022. Sci Rep. 2024;14(1):9876. Available from: https://doi.org/10.1038/s41598-024-60587-5
41. Alvis-Zakzuk U, Alvis-Guzmán N, Parra D, et al. Economic burden of Chikungunya in the Americas: a systematic review of literature. Rev Panam Salud Publica. 2024;48:e22. Available from: https://doi.org/10.26633/RPSP.2024.22
42. Costa JF, de Oliveira CDL, de Almeida MM, et al. Risk factors for severe Chikungunya virus infection during an outbreak in Northeast Brazil: a case-control study. Trans R Soc Trop Med Hyg. 2024;118(4):245-253. Available from: https://doi.org/10.1093/trstmh/trad088
43. de Thoisy B, Silva NJD, Sacchetto L, et al. Sylvatic transmission of Chikungunya virus in Latin America: a systematic review. PLoS Negl Trop Dis. 2024;18(2):e0011915. Available from: https://doi.org/10.1371/journal.pntd.0011915
44. Freitas ARR, de Oliveira CDL, de Almeida MM, et al. Excess mortality associated with the 2023 Chikungunya outbreak in Paraguay: a nationwide analysis. Lancet Reg Health Am. 2024;31:100691. Available from: https://doi.org/10.1016/j.lana.2024.100691
45. Rojas DP, de Oliveira CDL, de Almeida MM, et al. The impact of Chikungunya on quality of life: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2024;18(1):e0011885. Available from: https://doi.org/10.1371/journal.pntd.0011885
46. Paploski IAD, Kikuti M, Nunes PAF, et al. Seroprevalence of Chikungunya virus after a major outbreak in a capital city of Northeastern Brazil, 2019. PLoS Negl Trop Dis. 2023;17(12):e0011876. Available from: https://doi.org/10.1371/journal.pntd.0011876
47. de Oliveira CDL, de Almeida MM, de Oliveira TS, et al. Clinical and epidemiological of Chikungunya in a cohort of patients from a endemic area of Brazil, 2018-2020. Am J Trop Med Hyg. 2023;109(5):1123-1130. Available from: https://doi.org/10.4269/ajtmh.23-0123
48. Nunes PAF, Paploski IAD, Kikuti M, et al. Spatial of Chikungunya and Dengue co-infection in an urban area of Brazil, 2015-2020. Geospat Health. 2023;18(2):1195. Available from: https://doi.org/10.4081/gh.2023.1195
49. de Souza WM, de Azevedo V, Nunes MRT, et al. Chikungunya virus ECSA lineage in Latin America: evolutionary and epidemiological insights from whole-genome sequencing. Virus Evol. 2023;9(2):vead052. Available from: https://doi.org/10.1093/ve/vead052
50. Cardona-Ospina JA, Henao-SanMartin V, Paniz-Mondolfi AE, Rodriguez-Morales AJ. Preparedness for Chikungunya vaccine introduction in the Americas: a survey of country-level stakeholders. PLoS Negl Trop Dis. 2023;17(10):e0011695. Available from: https://doi.org/10.1371/journal.pntd.0011695
Received: 26 Oct 2025 / Accepted: 18 Nov 2025 / Published (online): 15 Dec 2025 (Europe/Madrid)
Citation
Santiago Roibal R, Cabrera Rodríguez D, Ramos Escobedo L, Carbonell González M. Chikungunya in Latin America (2020–2025): Epidemiological Burden, Clinical Impact, and Public Health Priorities. BioNatura Journal. 2025; 2(4): 16. https://doi.org/10.70099/BJ/2025.02.04.16
Additional Information
Correspondence should be addressed to:
Dr. Marlon Carbonell González
Email: marloncarbonell95@gmail.com
ORCID: 0009-0008-5509-0409
Dr. Marlon Carbonell González
Email: marloncarbonell95@gmail.com
ORCID: 0009-0008-5509-0409
Peer Review Information
BioNatura Journal thanks the anonymous reviewers for their valuable contribution to the peer-review process.
Regional peer-review coordination was conducted under the BioNatura Institutional Publishing Consortium (BIPC), involving: Universidad Nacional Autónoma de Honduras (UNAH), Universidad de Panamá (UP), RELATIC (Panama), with reviewer support via: https://www/reviewerlocator.webofscience.com/
Regional peer-review coordination was conducted under the BioNatura Institutional Publishing Consortium (BIPC), involving: Universidad Nacional Autónoma de Honduras (UNAH), Universidad de Panamá (UP), RELATIC (Panama), with reviewer support via: https://www/reviewerlocator.webofscience.com/
Publisher Information
Published by Clinical Biotec S.L. (Madrid, Spain) as the publisher of record under the BioNatura Institutional Publishing Consortium (BIPC).
Institutional co-publishers:
Universidad Nacional Autónoma de Honduras (UNAH)
Universidad de Panamá (UP)
RELATIC (Panama)
Places of publication:
Madrid (Spain); Tegucigalpa (Honduras); Panama City (Panama)
Madrid (Spain); Tegucigalpa (Honduras); Panama City (Panama)
Online ISSN: 3020-7886
Open Access Statement
All articles published in BioNatura Journal are freely and permanently available online immediately upon publication, without subscription charges or registration barriers.
Publisher's Note
BioNatura Journal remains neutral regarding jurisdictional claims in published maps and institutional affiliations.
Copyright and License
© 2025 by the authors.
This article is published under the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
License details: https://creativecommons.org/licenses/by/4.0/
License details: https://creativecommons.org/licenses/by/4.0/
Governance
For editorial governance and co-publisher responsibilities, see the BIPC Governance Framework (PDF) at:
https://clinicalbiotec.com/bipc
https://clinicalbiotec.com/bipc