Risk of renal dysfunction in patients with dengue fever: a case-control study

Waheed Haider 1, Kaleem Maqsood 1*, Husna Ahmad 1, Humera Naveed 1, Muhammad Amir Iqbal 1, Nabila Roohi 1,
1Institute of Zoology, University of the Punjab, Lahore; Pakistan
*Correspondence: kaleemmaqsood4@gmail.com
1Institute of Zoology, University of the Punjab, Lahore; Pakistan
*Correspondence: kaleemmaqsood4@gmail.com
ABSTRACT
Dengue fever, a mosquito-borne infection, is typically caused by the Dengue virus, leading to various illnesses, including dengue fever and severe dengue fever. This study aims to investigate the outcome of dengue fever severity as renal dysfunction in patients. For this case-control study, blood samples of the patients (N=66), including 31 D-W (Dengue without warning signs), 20 D+W (Dengue with warning signs), and 15 SDF (Severe dengue fever), as well as controls (N=45) of same age groups, were obtained. The renal parameters were determined and statistically analyzed using a one-way ANOVA and chi-square/Fisher exact test. The intergroup comparison showed that phosphorous, calcium, and sodium presented a marked decrease (P < 0.001) in dengue patient groups compared to controls. However, a significant increase (P < 0.05) in chloride was indicated in dengue patient groups.
Moreover, a prominent potassium reduction (P = 0.036) was observed in the dengue subjects group compared to controls. Among the renal parameters, creatinine presented a significant elevation (P < 0.002) while uric acid was significantly (P = 0.004) dropped in dengue patients groups as compared to controls. This study's results suggest that dengue infection's severity may be associated with aberrant electrolyte imbalance and renal impairment. This study indicates that dengue affects normal kidney functions and harms the patients' health.
Keywords: electrolytes; renal profile; dengue fever; severe dengue fever
INTRODUCTION
Dengue fever is a mosquito-borne disease caused by the dengue virus, with a range of clinical manifestations from a simple fever to more severe conditions such as dengue shock syndrome (DSS) and dengue hemorrhagic fever (DHF).1, 2
Over the last two decades, the number of dengue cases reported to the World Health Organization has seen an exponential rise, with the figure growin from 505,430 in 2000 to 2.4 million in 2010 and a staggering 5.2 million in 2019, representing an increase of more than eightfold while there was a dramatic increase in the number of confirmed casualties, particularly among younger age groups, rising from 960 to 4032 was also recorded. A significant dengue outbreak in Pakistan occurred between September and December 2019, resulting in 53,498 cases and 95 fatalities.3
The severity of dengue fever can vary from a mild fever to a more severe infection, such as hemorrhagic fever, which is often accompanied by shock, and typically, patients experience the sudden onset of fever, body aches, and headaches. A severe cold, pain in the eye sockets, joint pain, anorexia, vomiting, and nausea sometimes precede this.4 Patients also lack taste sensation, a mild sore throat, and, in some cases, constipation. In some cases, a cardiovascular condition such as bradycardia may be observed in patients two days after they have contracted this infection, as well as varying levels of bleeding.5
An individual's dengue infection can be confirmed when their platelet count in the blood drops to 100000/mm3, a crucial symptom of dengue fever. The decrease in blood platelet counts is evidenced by an increase in the permeability of the capillary, which is usually accompanied by an increase in the hematocrit value. This is accompanied by a reduction in the amount of protein present in the blood serum, which is observed to take place two or more days before the onset of hypovolemia.6 The body requires a range of electrolytes, such as phosphorus, chlorides, calcium, sodium, and potassium, to function optimally and maintain normal operations.7
The kidney is a vital organ in our body responsible for regulating the electrolyte level in the body, sustaining the volume of the extracellular fluid, maintaining the acid-base balance of the organism, and eliminating the metabolic byproducts of proteins. Any type of damage to the kidney results in the disturbance of all the blood components depending on its normal functioning.8
This study seeks to ascertain the consequences of dengue infection on the human body, including its potential associated risks. The primary objective is to evaluate the variations in the association of severity and renal dysfunction, as assessed by serum electrolytes and renal profile.
MATERIAL AND METHODS
For this case-control study, 111 subjects were recruited, fulfilling inclusion criteria; among them, 66 were dengue patients divided into different categories (31=D-W, 20=D+W, and 15=SDF) according to WHO criteria 9 from the Mayo Hospital, Lahore. In contrast, 45 healthy individuals of the same age groups were recruited as controls from the University of the Punjab, Lahore. The Institute of Zoology, University of the Punjab, Lahore's institutional review committee approved this study.
Before recruitment, all subjects were informed about this study, and written informed permission was taken. The subjects having comorbidities like diabetes, cancer, CVDs, etc., as well as smokers, were excluded. A detailed performance was designed to collect information on the subject, including the patient's clinical symptoms and socio-demographic data of all subjects.
A registered laboratory technician has assisted in collecting blood samples from the participants, utilizing sterilized syringes of Becton Dickinson to draw 5 ml of blood from each subject. Subsequently, the collected blood was poured into the labeled red serum tube containing the clot activator and transported to the Physiology laboratory, where the vials were left at room temperature for half an hour until clot formation. Afterward, the tubes were spun in a centrifuge at 4000rpm for 15 minutes. After centrifugation, serum was separated, poured into labeled Eppendorf, and stored at -80°C in the freezer until further analysis.
In the biochemical analysis, the phosphorous, chloride, and calcium concentrations were measured by ( Monlab kits). Meanwhile, Arena bioscience kits measured levels of sodium and potassium. The creatinine, urea, and uric acid levels were measured by (AMP diagnostic kits). Biochemical analysis was done using the automated (Robert Riele KG) photometer 5010 V5+ in the Physiology Laboratory, Institute of Zoology, University of Punjab Lahore.
Through One-Way ANOVA, they statistically analyzed the obtained results of serum electrolytes and renal profile to find the variations between the groups while the Chi-Square/Fisher Exact test for association of clinical symptoms with the severity of the fever at the significance level of P <0.05. This data analysis was done by using IBM-SPSS and GraphPad Prism software. The results were presented as mean ± SEM in tabular and graphical form.
RESULTS
Out of the total N=111 subjects, 45 were controls including 20(44%) males and 25(56%) females as well as 66 were dengue patients including 41(62%) males and 25(38%) females. All study subjects were aged 10-50 and categorized into groups (Table 1).

Table 1: Socio-demographic features of dengue patients and controls
Among the clinical symptoms, nausea, rashes, aches, and tourniquet tests were most prevalent in patients (Table 2, Fig 1). However, tenderness, vomiting, mild bleeding, lethargy, HCT increase, and medical intervention were rare and common in D+W and SDF patients (Table 2, Fig 2). In D-W patients, shock, respiratory distress, severe bleeding, and impaired consciousness were absent and linked with D+W and SDF (Table 2, Fig 3).
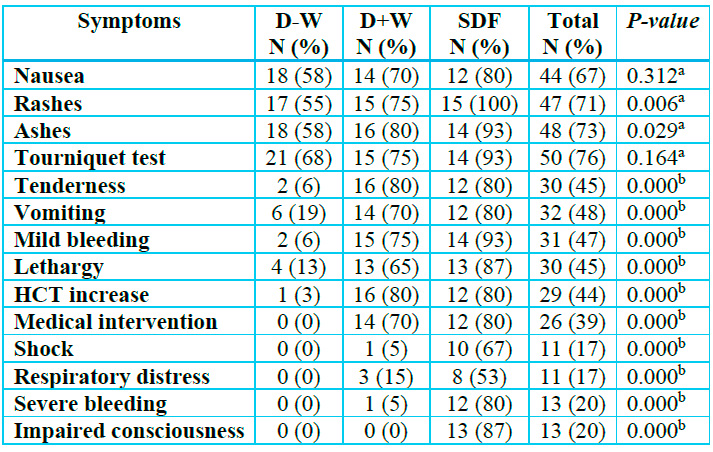
aChi-square test;b Fisher's exact test
Table 2: Frequency (%) of clinical symptoms among dengue patients with No Warning Signs (D-W), With Warning Signs (D+W), and Severe Dengue Fever (SDF).
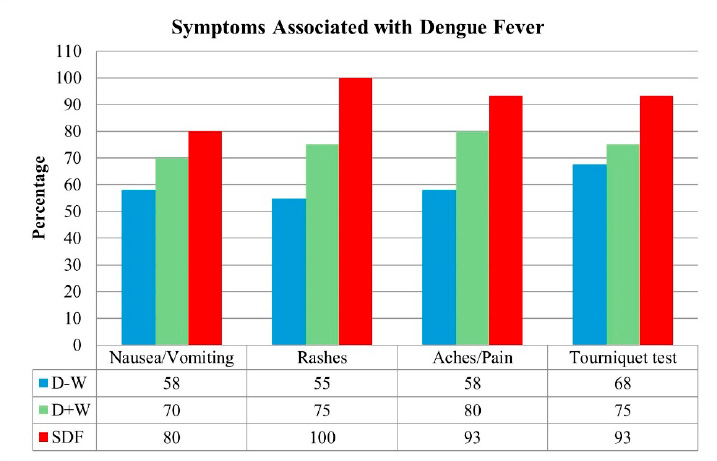
Figure 1: Represents the symptoms associated with dengue with no warning sign (D-W), dengue with warning signs (D+W), and Severe dengue fever (SDF).

Figure 2: Represents the symptoms associated with dengue with no warning sign (D-W), dengue with warning signs (D+W), and Severe dengue fever (SDF).

Figure 3: Represents the symptoms associated with dengue with no warning sign (D-W), dengue with warning signs (D+W), and Severe dengue fever (SDF).
Intergroup comparison of Mean ± SEM values of serum electrolytes level and renal profile between D-W, D+W, SDF, and controls were made through One-Way ANOVA. Among the electrolytes, phosphorus levels in the patients with D-W, D+W, and SDF decreased significantly (P≤0.001) as compared to controls (Table 3, Fig; 4A). Chloride levels in the patients with D-W, D+W, and SDF were increased significantly (P≤0.01) as compared to controls (Table 3, Fig; 4B). Calcium levels in the patients with D-W, D+W, and SDF decreased significantly (P≤0.001) as compared to controls (Table 3, Fig; 4C). Sodium levels in the patients with D-W, D+W, and SDF were decreased significantly (P≤0.001) as compared to controls (Table 3, Fig; 4D). Potassium levels in the patients with D-W, D+W, and SDF (3.46±0.36) decreased significantly (P≤0.05) as compared to controls (Table 3, Fig; 4E).
However, among the renal profile, creatinine levels in the patients with D-W, D+W, and SDF increased significantly (P≤0.01) in patients as compared to controls (Table 3, Fig; 4F). Urea levels in the patients with D-W, D+W, and SDF increased non-significantly in patients as compared to controls (Table 3, Fig; 4G). Uric acid levels in the patients with D-W, D+W, and SDF decreased significantly (P≤0.01) in patients as compared to controls (Table 3, Fig; 4H).

Table 3: Overall intergroup comparison of serum renal profile in control and patients with dengue fever with no warning signs (D-W), dengue with warning signs (D+W), and severe dengue fever (SDF).

Figure 4 (A-H): Intergroup comparison of Mean± SEM of serum renal profile in dengue patients having No Warning Signs (D-W), With Warning Signs (D+W), and Severe Dengue Fever (SDF) with controls. *,**,*** represent the significance at P≤0.05, 0.01, and 0.001, respectively.
DISCUSSION
Imbalances in the levels of electrolytes and other substances commonly found in the kidneys can lead to serious health problems that can affect the body's metabolism and functioning. The transmission of nerve impulses, muscle movement, and maintaining body homeostasis are all vital functions dependent upon these electrolytes. Variations in the electrolytes present in the body can lead to symptoms such as impaired nerve impulse transmission and altered muscle movement. The levels of electrolytes in the body's serum are widely used as indicators of renal dysfunction, and disturbances in the body's electrolyte balance can also cause renal dysfunction.10
The presence of the dengue virus in the body can lead to various renal issues, such as an elevation of serum creatinine, acute kidney injury, acute tubular necrosis, hemolytic uremic syndrome, proteinuria, and nephrotic syndrome.11
In this study, it was observed that the sodium level in the patients was significantly lower than the normal level. The average amount of sodium in the serum of those with dengue infection was notably lower than that of healthy individuals. Hyponatremia may be caused by an abundance of water resulting from an increased metabolic rate, a lack of salt, a decrease in renal excretion, inappropriate secretion of antidiuretic hormone from the pituitary gland, an abnormal sodium-potassium pump leading to sodium entering cells, and sodium is lost in the urine due to acute tubular necrosis. The swelling of the brain due to hyponatremia is the primary factor responsible for convulsions in individuals suffering from dengue infection.12
Hyponatremia is commonly caused by conditions such as diarrhea, diuretics, abnormal secretion of the antidiuretic hormone from the pituitary gland, and dysfunction of the kidneys.13 Patients with dengue infection typically exhibit a mild decrease in sodium concentration in their blood.14
In this investigation, it was observed that the amount of calcium in the blood serum of individuals suffering from dengue was significantly lower than that of individuals in the control group.
Patients suffering from dengue fever may experience hypocalcemia, which can be attributed to a decrease in the activity of the Na+/K+ ATPase pump, the Ca2+ ATPase pump, and the acquisition of a deficiency in parathyroid hormone. This reduced trend of calcium in our investigation is per the study of Hira Kaur 15.
There is a correlation between hypocalcemia and cardiovascular abnormalities, such as low blood pressure and decreased performance of the heart muscle. Disruptions in the calcium concentration of the blood may cause signs and symptoms of illness associated with hypocalcemia, which is characterized by cardiovascular or neuromuscular dysfunction 16. Hypocalcemia has been identified as a biomarker of organ failure and the severity of dengue and has been linked to myocarditis and cardiac dysfunction caused by the disruption of intracellular calcium levels.17
Compared to normal subjects, patients with dengue infection have a significantly lower serum phosphate level. The potential causes of hypophosphatemia may include the utilization of diuretics, the administration of antacids, the intravenous infusion of a glucose solution, the occurrence of diarrhea, the occurrence of vomiting, and the presence of kidney dysfunction. Hypophosphatemia can lead to a range of serious complications, including hemolytic anemia, acute respiratory failure, severe muscle weakness, heart failure, and even coma.18
Our study revealed that the amount of potassium in the blood serum of individuals with dengue infection was significantly lower than that of healthy individuals. Hypokalemia is primarily caused by an abnormal distribution of potassium within cells, abnormalities in the renal tubules, which lead to excessive potassium loss in the urine, and an elevation of the renin hormone in the serum. An abnormally low potassium level in the body may cause vomiting, diarrhea, and other symptoms such as muscle weakness, fatigue, heart palpitations, and muscle spasms.19
The chloride levels in the body serum of patients are significantly higher than those of healthy individuals. Hyperchloremia correlates with fatigue, an increased desire for fluids, elevated blood pressure, and decreased muscular strength. The primary factor leading to renal impairment is a high chloride level in the bloodstream resulting from intravenous fluids.20
The precise indicators for ascertaining the regular operation of the kidneys are the creatinine and uric acid levels in the body's serum, as the kidneys excrete these substances. The serum creatinine levels of the patients with dengue infection have been notably higher than those of the individuals in the healthy group. The decreased efficiency of kidney function is the cause of the increased concentrations of creatinine and uric acid in the blood.21
Elevated creatinine levels can lead to severe renal dysfunction and other symptoms 22. In the study, Akomolafe, Adeoshun 23 observed that elevated creatinine level has a more destructive effect on kidney function. A different study found that the amount of creatinine in dengue patients decreased, which does not align with the results of my research.24
The body urea level of the patients was not significantly higher than that of the healthy subjects. Elevation of urea in the body is primarily caused by an excessive loss of fluid resulting from renal infection. Uremia is a condition in which the urea levels in the body are abnormally high, leading to a range of symptoms, including coma, cardiac arrest, and death. This heightened level of urea can cause the kidneys to become swollen, enlarged, congested, and potentially hemorrhagic, causing congestion and edema in the patient. Diet, dehydration, and antidiuretic medicines are also causes of the increase in the level of urea in the serum.23
The concentration of uric acid in the bodies of individuals suffering from dengue is lower than that of individuals unaffected by the disease. Uric acid is the most critical antioxidant in the blood. It has been observed that the concentration of uric acid in individuals suffering from dengue fever has been reduced by up to 1.5 times. The reduction of uric acid levels in patients with DHF leads to a decrease in their body's natural antioxidant defense system, increasing oxidative stress. A decreased amount of uric acid in the body's serum has been linked to various complex conditions caused by an imbalance in the production of oxidizing agents and a decrease in the body's natural antioxidant defenses.25
The small sample size and focus on a specific geographic area may limit the generalizability of the findings. Future studies with larger, diverse samples and broader renal assessments are needed to confirm and expand on these findings.
CONCLUSIONS
In conclusion, we can say that dengue infection can have severe consequences on human health, particularly affecting the kidneys and causing renal dysfunction. The disease leads to significant changes in electrolyte levels and renal biomarkers. Without preventive measures, individuals may experience kidney problems and electrolyte imbalances. To prevent dengue infection, it is recommended to use mosquito repellent, wear protective clothing, and control mosquito populations. Improving case management and early detection of dengue symptoms are crucial in reducing mortality rates associated with the disease.
Author Contributions: WH: Biochemical analysis. KM: Blood sampling and data collection. HA: statistical analysis. HN: scientific writing and interpretation of data. MAI: Design the work and substantive revisions of the paper. NR: Supervision and final revision. All authors read and approved the final manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: Approved by the Institutional Review Committee of the Institute of Zoology, University of the Punjab, Lahore. The study was performed per the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent Statement: Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement: The data used in this study are available upon request from the corresponding author. Due to privacy and ethical considerations, some restrictions may apply to the availability of specific sensitive or confidential data. Requests for access to the data will be considered on a case-by-case basis, subject to any necessary ethical and legal approvals.
Acknowledgments: We thank the Institute of Zoology, University of the Punjab, Lahore, for providing the necessary facilities and support for this research.
Conflicts of Interest: The authors declare that they have no conflicts of interest related to this
REFERENCES
1. Arora M, Patil RS. Cardiac manifestation in dengue fever. J Assoc Physicians India. 2016;64(7):40-4.
2. Araújo SA, Moreira DR, Veloso JMR, Silva JO, Barros VLSR, Nobre V. Case report: fatal staphylococcal infection following classic dengue fever. The American journal of tropical medicine and hygiene. 2010;83(3):679.
3. WHO. Dengue fever – Pakistan: World Health Organization; 2021 [updated December 14 2021. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/dengue-fever-pakistan.
4. Schaefer TJ, Panda PK, Wolford RW. Dengue fever. 2017.
5. Waterman SH, Gubler DJ. Dengue fever. Clinics in dermatology. 1989;7(1):117-22.
6. Halstead SB. Pathophysiology and pathogenesis of dengue haemorrhagic fever. Monograph on dengue/dengue haemorrhagic fever New Delhi: World Health Organization. 1993:80-103.
7. Ochei JO, Kolhatkar AA. Medical laboratory science: theory and practice: McGraw Hill Education; 2000.
8. Schöttker B, Brenner H, Koenig W, Müller H, Rothenbacher D. Prognostic association of HbA1c and fasting plasma glucose with reduced kidney function in subjects with and without diabetes mellitus. Results from a population-based cohort study from Germany. Preventive medicine. 2013;57(5):596-600.
9. Hakovirta H, Syed V, Jégou B, Parvinen M. Function of interleukin-6 as an inhibitor of meiotic DNA synthesis in the rat seminiferous epithelium. Molecular and cellular endocrinology. 1995;108(1-2):193-8.
10. Gurugama P, Jayarajah U, Wanigasuriya K, Wijewickrama A, Perera J, Seneviratne SL. Renal manifestations of dengue virus infections. Journal of Clinical Virology. 2018;101:1-6.
11. Mallhi TH, Khan YH, Adnan AS, Tanveer N, Aftab RA. Dengue-Induced Renal Complications. Expanded Dengue Syndrome: Springer; 2021. p. 35-54.
12. Mekmullica J, Suwanphatra A, Thienpaitoon H, Chansongsakul T, Cherdkiatkul T, Pancharoen C, et al. Serum and urine sodium levels in dengue patients. Southeast Asian J Trop Med Public Health. 2005;36(1):197-9.
13. Patil VC, Botre A, Patil R. Study of Electrolyte Disturbances in Dengue Infected Patients. 2019.
14. Anwar T, Rais H, Saba Safdar SE. Altered Electrolyte Homeostasis and the Severity of Dengue in Children.
15. Hira HS, Kaur A, Shukla A. Acute neuromuscular weakness associated with dengue infection. Journal of neurosciences in rural practice. 2012;3(01):36-9.
16. Kelly A, Levine MA. Hypocalcemia in the critically ill patient. Journal of intensive care medicine. 2013;28(3):166-77.
17. Singh AR, Dnyanesh D. The prevalence of hypocalcemia in children with dengue infection: A 1-year cross-sectional study. Indian Journal of Health Sciences and Biomedical Research (KLEU). 2019;12(2):166.
18. Halevy J, Bulvik S. Severe hypophosphatemia in hospitalized patients. Archives of Internal Medicine. 1988;148(1):153-5.
19. Jha S, Ansari M. Dengue infection causing acute hypokalemic quadriparesis. Neurology India. 2010;58(4):592.
20. Ismail J, Sankar J. Acute Kidney Injury in Dengue–Not Unprecedented. The Indian Journal of Pediatrics. 2020;87(12):993-4.
21. Haschek W, Winder C. Occupational toxicology of the kidney. Occupational toxicology: CRC Press; 2004. p. 153-67.
22. Hasannia T, Moosavi Movahed SM, Vakili R, Rafatpanah H, Hekmat R, Valizadeh N, et al. Active CMV and EBV infections in renal transplant recipients with unexplained fever and elevated serum creatinine. Renal Failure. 2016;38(9):1418-24.
23. Akomolafe R, Adeoshun I, Fakunle JB, Iwalewa E, Ayoka A, Ajayi O, et al. Changes in some biochemical parameters of kidney functions of Plasmodium berghei infected rats administered with some doses of artemether. African Journal of Biotechnology. 2012;11(27):7119-27.
24. Mehboob R, Syed AS, Bukhari MH, Khan AA, Ahmad FJ. Predictors for severity of dengue infection during early days of infection. Walailak Journal of Science and Technology (WJST). 2012;9(4):369-74.
25. Cui L, Pang J, Lee YH, Ooi EE, Ong CN, Leo YS, et al. Serum metabolome changes in adult patients with severe dengue in the critical and recovery phases of dengue infection. PLoS neglected tropical diseases. 2018;12(1):e0006217.
Received: May 17, 2023 / Accepted: September 30, 2024 / Published: December 15, 2024
Citation: Haider W, Maqsood K, Ahmad H, Naveed H, Iqbal MA, Roohi N. Risk of renal dysfunction in patients with dengue fever: a case-control study Bionatura journal. 2024;1(4):12. doi: 10.70099/BJ/2024.01.04.12
Additional information Correspondence should be addressed to kaleemmaqsood4@gmail.com
Peer review information. Bionatura thanks anonymous reviewer(s) for their contribution to the peer review of this work using https://reviewerlocator.webofscience.com/
ISSN.3020-7886
All articles published by Bionatura Journal are made freely and permanently accessible online immediately upon publication, without subscription charges or registration barriers.
Publisher's Note: Bionatura Journal stays neutral concerning jurisdictional claims in published maps and institutional affiliations.
Copyright: © 2024 by the authors. They were submitted for possible open-access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).