


Clinical and Thermographic Evaluation of the Inflammatory Response to Third Molar Removal

Jéssica Hálice Noronha 1*, Denise Sabbagh Haddad 2, Leandra Ulbricht ¹, Bruna Martini ³,
André Luis Zetola ³, Eduardo Borba Neves ¹
¹ Graduate Program of Biomedical Engineering, Federal Technological University of Paraná (UTFPR),
Paraná, Brazil.
² Department of Stomatology, School of Dentistry, University of São Paulo (FOUSP), São Paulo, Brazil.
³ Graduate Program of Oral and Maxillofacial Surgery, Positivo University Curitiba, Paraná, Brazil.
Corresponding author. noronhajessicahalice@gmail.com
Paraná, Brazil.
² Department of Stomatology, School of Dentistry, University of São Paulo (FOUSP), São Paulo, Brazil.
³ Graduate Program of Oral and Maxillofacial Surgery, Positivo University Curitiba, Paraná, Brazil.
Corresponding author. noronhajessicahalice@gmail.com
ABSTRACT
This study aimed to compare two different drug protocols to be used during the preoperative period, consisting of different corticoids and with various routes of administration. An observational and longitudinal study was carried out with 30 volunteers who needed the removal of impacted or semi-impacted third molars in the mandible region. Volunteers were equally divided into two groups, with the drug protocol administered in the preoperative phase, one hour before surgery. Two protocols were used: Dexamethasone 8.0 mg orally (VO) and Betamethasone Dipropionate 5mg/mL + Betamethasone Disodium Phosphate 2mg/mL intramuscularly (IM). Postoperative medication was standard for both groups. The volunteers were monitored in the pre- and postoperative periods (third and seventh days). Local temperature, maximum mouth opening, edema, and pain were evaluated. With regard to the skin temperature response, significant effects were identified for the interaction between the moment in which the evaluations were carried out and the corticoid administered in the following regions of interest and analyzed temperatures: Operated mandibular angle (maximum (F(2, 56)=3.89, p=0.026, ηp2=0.122), mean (F(2.56)=3.47, p=0.038, ηp2=0.110) and minimum (F(2.56)=4.03, p=0.023, ηp2=0.126)) and in the Control =0.116 )). The Betamethasone IM group showed an increase in skin temperature on the third postoperative Mandibular Angle (maximum (F(2.56)=3.36, p=0.042, ηp2=0.107), and minimum (F(2.56)=3.66, p=0.032, ηp2day. In evaluating pain, edema, and maximum mouth opening, a similar behavior tendency was noticed in both drug protocols. It can be concluded that dexamethasone 8.0mg VO and Betamethasone dipropionate 5mg/mL + betamethasone disodium phosphate 2mg/mL IM did not present significant differences in edema, pain, and limitation of mouth opening in the postoperative period when compared, concerning skin temperature, there was a difference when considering the absolute temperature. Considering the results of this study, Dexamethasone is recommended as a preoperative protocol for removing third molars.
Keywords: Thermography; Surgery; Impacted third molar; Corticosteroids; Inflammatory response.
INTRODUCTION
Surgery to remove third molars is common in dental offices and generates mechanical trauma during the procedure, especially in cases where these dental elements are semi-impacted or impacted1, 2. Pain, edema, and limited mouth opening are the main postoperative complaints reported by patients undergoing this procedure 1, 3.
The inflammatory response causes the symptoms to form part of the organism's defense mechanism when submitted to an injury in its tissues and has a defensive character1, 4, 5. The drug protocols used with anti-inflammatory power aim to decrease the exacerbation of this inflammation1, 2. Preoperative administration of corticosteroids significantly decreases facial edema in surgeries to remove third molars; this has been previously documented in systematic reviews and is routinely used as a protocol in dental services1,6,7.
Glucocorticoids are classified according to their duration and potential for action8. Dexamethasone is a potent glucocorticoid with a long half-life, interrupting the inflammatory cascade in the early stages 5. The literature does not show a consensus regarding studies that analyze the inflammatory response in terms of dosage and delivery route with greater efficiency for its use in the period before surgery. However, one study showed a tendency to use Dexamethasone, methylprednisolone, and Betamethasone orally, intramuscularly, and intravenously in oral surgeries1, 9.
Betamethasone, in turn, matches Dexamethasone in terms of potency and half-life1. Both are rated with high potency, prolonged potency, and length of action1
A review published by authors Ngeow and Lim6 reported that for some unknown reason, few studies have attempted to compare the effectiveness of two different groups of corticosteroids. This is supported by the systematic review published by Larsen MK et al. 1 and the study published by Rabelo and Gomes8, which reviewed studies concluding that the optimal dosage and administration route to decrease postoperative sequelae of lower third molar removal currently still leaves room for doubt and that more well-designed clinical studies are needed.
Some clinical indicators are used for the postoperative follow-up of removal and impacted third molars; among them is the measurement of maximum mouth opening using millimeter rulers measuring the interincisal distance; this is a functional aspect indicator, facial arches to measure edema are also utilized and visual pain scale (VAS) to quantify the level of pain during the postoperative inflammatory process 5.
Recently, thermal imaging has been applied in several areas of dentistry with great success and advantages such as low cost, portability, and ease of interpretation and not only to assess changes in temperature within the oral cavity but also to correlate tissue temperatures on the body surface with the condition of tissues within the oral cavity, to predict the outcomes of performed procedures2. Infrared thermography is a functional imaging method without the emission of ionizing radiation, fast and reflects the microcirculatory dynamics of the skin surface, capable of providing health professionals with objective and accurate information about the facial vasomotor and neurovegetative system and responses to tooth pain of inflammatory origin10.
Therefore, this study aims to investigate the signs of the inflammatory process in the postoperative period of impacted and semi-impacted third molar extractions in patients who used an oral Dexamethasone or an intramuscular Betamethasone Dipropionate + Betamethasone Disodium Phosphate drug protocol.
MATERIAL AND METHODS
The sample consisted of 30 patients of both genders, aged between 15 and 35 years, with previous indications of third molar extraction. All patients signed the Informed Consent Form (the project was registered and approved at Plataforma Brasil under number CAAE 48596621.0.0000.5547).
This study included patients who sought Oral and Maxillofacial Surgery and Traumatology services at a university located in Curitiba who had semi-impacted or impacted third molars in the mandible. Patients who had erupted third molars in the maxilla, therefore not requiring osteotomy or tooth section, had these teeth removed in the same procedure, not exceeding 5 minutes to complete the procedure.
The patients excluded from the study were those who had other impacted dental elements; had a history of allergy to the proposed drug protocols; smokers who had smoked their last cigarette within three hours of the procedure; pregnant women; patients taking continuous medication (except contraceptives); patients with systemic diseases; patients who scored more than 0 on the visual analog pain scale (VAS) preoperatively, characterizing possible prior inflammation in this dental element and patients requiring intravenous sedation for the procedure.
Drugs administered preoperatively
The protocols used by the Oral and Maxillofacial Surgery and Traumatology service where the volunteers were recruited were studied as observational research.
The research participants were randomly divided into two groups, with 15 participants each. Group A used the preoperative medication dexamethasone 8.0 mg (2 tablets of 4.0mg), and group B used intramuscular application of betamethasone dipropionate + betamethasone disodium phosphate 5mg/mL + 2mg/mL. The medication was administered 01 hours before surgery in both groups.
Surgical procedure
The procedure consisted in the removal of the impacted lower third molar and erupted upper third molar (when present), under local anesthesia, following the steps of the standard operative technique, being incision, followed by detachment, osteotomy, odontosection using a high rotation drill, dislocation of the tooth, cleaning of the cavity, irrigation and suture.
The patients were instructed to rinse for 60 seconds with chlorhexidine 0.12%, after which an extra-oral asepsis was performed with iodine. Local anesthesia was then performed using the pterygomandibular technique, with mepivacaine hydrochloride 2% and epinephrine 1:100,000. A relaxing incision in the retromolar region, detachment followed by osteotomy and odontosection (when necessary) using high rotation and dislocation of the dental element. The alveolar region was irrigated and prepared for synthesis with a 4.0 nylon suture.
The standardized prescription for the postoperative procedure was Amoxicillin 500 mg every eight hours for seven days, Ibuprofen 600mg granulated powder every eight hours for three days, and paracetamol 750mg every eight hours for three days. For hygiene of the region, 0.12% chlorhexidine mouthwash was prescribed every 12 hours for 7 days, starting 24 hours after the surgical procedure and orientation regarding brushing and postoperative care.
Evaluation protocols used
The evaluations performed were: Anamnesis (with identification of the volunteer, current and past medical and dental history), visual analog pain scale (VAS); thermographic analysis; measurement of maximum mouth opening, using a sterile ruler. The reference points were the incisal edge of the dental elements of the upper central incisor and lower central incisor. The measurement of maximum mouth opening did not exceed 2 seconds, thus avoiding as much as possible the painful exposure of the patient, besides the edema that was evaluated through observational quantitative analysis by one of the researchers comparing visible asymmetry with the contralateral side, being level 1 imperceptible, level 2 slightly asymmetric and 3 visible asymmetry. Three evaluations were performed: pre-surgical and on the third and seventh day, as well as the minimum, average, and maximum temperatures of the regions of interest (ROI).
Protocol for the infrared thermography examination.
The THERMACAM T540® Camera (Flir Systems®, USA) was used. The precautions prior to the evaluations involved avoiding the application of topical agents in the head and neck region; not using the hair dryer, flat iron, or any type of headband that would compress the head region on the day of the evaluation; no smoking, avoiding hot baths or showers less than 2 hours before the exam; not fasting for more than 3 hours before the exam; male patients removing their beard on the day before the evaluation.
The examination room was kept at 19°C (monitored by a thermometer positioned far from heat sources, preventing thermal losses by forced air convection directly over the volunteer). The relative humidity was kept between 50% and 70%. The participant was acclimatized for 20 minutes before the first thermal evaluation.
The camera was placed on a tripod 1.0 meters away from the participant in a standing position, and three images of the face were taken at each evaluation: one frontal and two lateral images (right and left).
Thermographic image analysis
For the analysis of the thermographic images, four (4) regions of interest were used: two standardized points in the mentual region (Figure 1) and two other points in the mandibular angle region (Figure 2). The analysis was performed using a comparative method, using the contralateral side as Control between the evaluation moments.

Figure 1. Region of interest (ROI) in the central area on the side with intervention performed and control ROI in the contralateral mandibular angle.

Figure 2. Points in mandibular angle regions and region of interest (ROI) on the side with intervention performed and control ROI in contralateral mandibular angle.
Statistical Analysis
The data were compiled and analyzed using Jamovi software (version 2.3.1). Line graphs with average and standard deviation representations were used to present the values obtained in the evaluations. The behavior of the variables studied was analyzed by analysis of variance (ANOVA) for repeated measures (2 groups x 3 time points).The partial squared eta (ηp2) was used to evaluate the power of the effect (effect size). The comparison of the variation of the deltas, for each temperature, between the evaluation times was performed by one-way ANOVA with Tukey's post hoc test. The deltas of each temperature between groups at each time point were compared using the Student's T-test. The significance level was set at 5% (α = 0.05).
RESULTS
The behavior of the thermal response of the skin indicates that the subjects who used Betamethasone IM showed an elevation of the skin temperature on the third postoperative day in the analysis of absolute temperatures through the analysis of variance. The volunteers who used oral Dexamethasone showed reduced skin temperature in all regions studied, considering absolute temperatures (Figure 3).

Figure 3. Behavior of the thermal response of the skin preoperatively, 3 days and 7 days postoperatively after extraction of impacted and semi-impacted third molars in patients who received different corticosteroids (Oral Dexamethasone or Betamethasone IM) preoperatively.
The behavior of the variables studied was considered by analysis of variance (ANOVA) for repeated measures. Regarding the response to skin temperature, significant effects were identified for the interaction between the time at which the evaluations were performed and the corticosteroid administered (Table 1 and Figure 3), in the following regions of interest and temperatures analyzed: Operated mandibular angle (maximum (F(2,56)=3.89, p=0.026, ηp2=0.122), average (F(2,56)=3.47, p=0.038, ηp2=0.110) and minimum (F(2,56)=4.03, p=0. 023, ηp2=0.126)) and in the mandibular angle Control (maximum (F(2,56)=3.36, p=0.042, ηp2=0.107), and minimum (F(2,56)=3.66, p=0.032, η2 ηp2=0.116)).

Caption: Mom * Cort = Interaction moment of evaluation + corticoid.
Table 1. Results of variance analysis (ANOVA) for repeated measures of the behavior of the thermal response of the skin, preoperatively, 3 days and 7 days after the extraction of semi-included and included third molars in patients who received different corticoids (Oral Dexamethasone or Betamethasone IM) preoperatively.
Table 2 compares the thermal asymmetry between the operated and Control sides (Delta). Table 3 presents the data comparing the thermal asymmetry between the operated and Control sides (Delta), when the corticoid groups patients used preoperatively. No significant differences were observed in the temperature delta between the groups stratified by the corticoid used preoperatively.
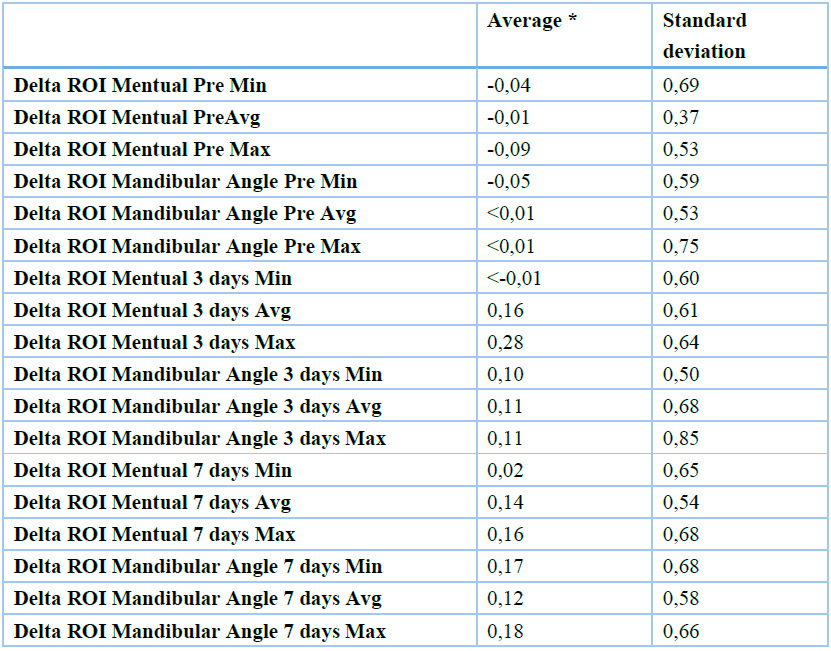
Caption:* The comparison of the variation of the deltas of each temperature at each moment of evaluation by one-way ANOVA indicated non-significant variation (p-value ranged from 0.05 to 0.92); Min=Minimum; Avg=Average; Max=Maximum.
Table 2.Thermal asymmetry between the operated side and the control side (Delta) of the 30 patients evaluated preoperatively, 3 days and 7 days after surgery for extractions of impacted and semi-impacted third molars in patients who received different corticosteroids (Oral Dexamethasone or Betamethasone IM) preoperatively.

Caption: Min=Minimum; Avg=Average; Max=Maximum
Table 3 . Comparison of thermal asymmetry between the operated side and the control side (Delta), preoperatively, at 3 days and 7 days postoperatively, in patients who received different corticosteroids (Oral Dexamethasone or Betamethasone IM) preoperatively, when the corticosteroid groups patients used preoperatively.
Figure 4 shows the behavior of the response on the visual analog scale for pain (VAS) -, mouth opening, and edema. The results presented in Table 4 indicate that there was an effect of the moment factor for the variables: pain (F(2,56)=3.51, p=0.037, ηp2=0.111), mouth opening (F(2,56)=20.858, p<0.001, ηp2=0.427) and edema (F(2,56)=141.96, p<0.001, ηp2=0.835). However, there was no significant difference in the behavior of pain, maximum mouth opening, and edema when considering the drug protocol used.

Figure 4. The behavior of the response on the visual analog scale (VAS) for pain, edema, and maximum mouth opening, preoperatively, 3 days and 7 days after the extraction of impacted and semi-impacted third molars in patients who received different corticoids (OralDexamethasone or Betamethasone IM) preoperatively.

Caption: Mom * Cort = Interaction moment of evaluation + corticoid, VAS = Visual Analog Scale.
Table 4 - Results of the analysis of variance (ANOVA) for repeated measures of the behavior of the visual analogue scale (VAS) for pain, edema, and maximum mouth opening in the preoperative period, at 3 days and 7 days after the extraction of impacted and semi-impacted third molars in patients who received different corticoids (Oral Dexamethasone or Betamethasone IM) preoperatively.
DISCUSSION
The objective of this research was to investigate the signs of the inflammatory process in the postoperative period of third molar extractions of impacted and semi-impacted third molars in patients who used a drug protocol with oral Dexamethasone 8.0 mg or intramuscular betamethasone dipropionate + betamethasone sodium phosphate 5mg/mL + 2mg/ML.
Corticotherapy in the preoperative period effectively controls edema and limits mouth opening due to inhibition of the conversion of phospholipids into arachidonic acid by phospholipase A2. This mechanism prevents the production of leukotrienes, prostacyclins, prostaglandins, and thromboxane A2, which mediate pain and inflammation. It is believed that corticosteroids can inhibit the initial step of this process1, 4, 5.
Although the two medications used in this research have great proximity of anti-inflammatory potential and time of action6. The results of this study indicate, through the analysis of absolute temperature, that the subjects who used Betamethasone IM showed an elevation of skin temperature on the third postoperative day, while the volunteers who used oral Dexamethasone showed a slight reduction in skin temperatures in most regions studied (interaction between time and corticosteroid administered, ANOVA for repeated measures, Table 1, Figure 3).
The factors that could explain this interaction moment vs. corticoid used in the surface thermal response are: pharmacokinetics (route of administration, absorption, distribution, and metabolism) and pharmacodynamics (drug action on enzymes, proteins, and cell receptors).
Comparing the absorption data and biological half-life of the two corticoids used in this study in association with the results presented in Figure 3, it can be inferred that the high speed of action of Dexamethasone administered orally was able to keep skin temperature stable in the ROIs evaluated. The effect of betamethasone dipropionate is observed in the thermal response of the skin between the third and seventh postoperative day (Figure 3).
In a study by Venta et al.12, the authors reported differences of less than 0.9°C comparing the operated side with the non-operated side the day after surgery, using a preoperative drug protocol, in a sample of 30 patients with a median age of 26 years and removal of an impacted third molar. The side with the highest temperature was the operated side. These results are higher than the values observed in the present study, which found differences in the average temperature between the operated and Control sides of less than 0.3°C on the third postoperative day (Table 2). The temperature deltas remained with similar values throughout the studied period (Table 2, one-way ANOVA, p>0.05). This fact can be explained by the systemic effect of the drugs used to control inflammation in the postoperative period (corticoid + anti-inflammatory)8, and by the action of the autonomic nervous system that seeks body thermal symmetry11. This fact has been previously reported in studies by other authors in the dental12.
Similarly, when the corticoid groups patients used preoperatively (Table 3), there were no significant differences in the temperature deltas between the groups (Student's T-test, p-value ranging from 0.071 to 0.903). However, an effect of the interaction moment + corticoid was observed in the absolute temperatures of the ROI of the Operated Mandibular Angle (maximum (F(2,56)=3.89, p=0.026, ηp2=0.122), average (F(2,56)=3.47, p=0.038, ηp2=0.110) and minimum (F(2,56)=4.03, p=0.023, ηp2=0. 126)) and in the ROI of the Control mandibular angle (maximum (F(2,56)=3.36, p=0.042, ηp2=0.107), and minimum (F(2,56)=3.66, p=0.032, ηp2=0.116)). In the study by Christensen et al., (2014), with 124 patients who had their third molar removed and the contralateral side was used as a control, thermography was performed on day 3 after surgery to analyze the temperatures in the group that used corticoid preoperatively and in the group that did not, they also found no significant difference between the groups (p=0.09), finding deltas for the average temperature on the order of 0.21ºC for the group that used corticoid and 0.39ºC for the control group.
This effect of the interaction moment of evaluation + corticoid can be explained by differences in pharmacokinetics and pharmacodynamics of corticoids used preoperatively. In 2013, Boonsiriseth et al. 13 reported a similar approach to the present study that compared the efficacy of intramuscular Dexamethasone and oral Dexamethasone, seeking to reduce sequelae of third molar surgery. They found no significant difference between the two groups, agreeing with the study by 14 that both routes of administration were equivalent in reducing the sequelae of third molar surgery. Oral Dexamethasone is rapidly and completely absorbed from the gastrointestinal tract. It reaches its maximum effect after oral administration in 1 to 2 hours, and its action lasts 1.25 to 1.5 days. The plasma half-life of Dexamethasone is 150 to 270 minutes, while the biological (tissue) half-life is 24 to 72 hours. The metabolism of Dexamethasone occurs in the liver and other cells, and its excretion occurs through urine. Almost all metabolites are excreted after 72 hours of its ingestion 15.
Betamethasone Dipropionate + Betamethasone Disodium Phosphate IM, the reference drug, is Diprospan, associated with betamethasone esters that produce an anti-inflammatory effect. The immediate therapeutic activity is provided by the soluble ester, betamethasone disodium phosphate, which is rapidly absorbed after administration, its plasma half-life is 3 to 5 hours, and the biological (tissue) life span is 36 to 54 hours. Its maximum effect is reached in 1 to 2 hours after administration, with the duration of action extended to 3.25 days16. Betamethasone undergoes hepatic biotransformation, and excretion occurs through urine16.
The different injectable corticosteroids (CCT) are synthetic analogs of cortisol. Their pharmacodynamics are not yet fully understood. Several mechanisms have been suggested: limitation of capillary dilation and permeability; decreased accumulation of polymorphonuclear leukocytes and macrophages; reduced release of vasoactive kinins; inhibition of catalytic enzyme release; inhibition of phospholipase A2, with reduced arachidonic acid release from phospholipids and consequent decreased formation of leukotrienes and pro-inflammatory prostaglandins, such as prostacyclin 17.
Structurally, Betamethasone is analogous to Dexamethasone and is marketed in free form and as acetate, benzoate, dipropionate, sodium phosphate, and valerate. In the free form, it is administered orally or topically, and the phosphate sodium esters can be given by intramuscular injection. 18.
The rate of action of intramuscular injectable drugs is highly dependent on drug release from the formulation and absorption from the injection site. Variables that affect drug release and absorption after injection include aspects of the pharmaceutical formulation, e.g., initial drug concentration and physicochemical properties of the drug. Biopharmaceutical aspects, e.g., route of administration, injection site, injection technique, and depth of injection18.
Regarding the interaction between corticosteroid + nonsteroidal anti-inflammatory drugs (NSAIDs), a study shows that the combination of a corticosteroid with NSAID is often more effective in controlling postoperative pain and edema than a NSAID alone 1, 8, agree that corticosteroids supplement NSAIDs regarding the blocking of edema as well as Moore et al, who in 2005, in their study revealed that Dexamethasone reduced trismus and edema and, associated with Rofecoxib, had even more expressive and positive results. This shows that old studies are supported by current articles in the sense that the interaction of corticoid and nonsteroidal anti-inflammatory drugs is effective in controlling inflammatory cardinal signs in the postoperative period.
In the present study, for the pain variable, evaluated by the Visual Analog Scale (VAS), an effect of the moment (Table 4, F(2,56)=3.511, p 0,037, ηp2=0.111), with an elevation on day 3 and remained linear from day 3 to day 7 and with similar behavior in both groups (stratified by corticoid used preoperatively)(F(1,28)=0,009, p 0.922, ηp2=0.000). This last result agrees with the findings of Silva MC et al., 2020, who compared Dexamethasone and Betamethasone, both 4mg orally, in 40 patients with an average age of 18 to 35 years and reported that no differences were found between the two protocols in the pain variable (p=0.819), the method used for analysis was the same as this work, i.e., visual scale (VAS)19. Al-Shamiri et al, published a research in 2017 comparing a group using Dexamethasone 8.0 mg (02 tablets of 4mg) 1 hour before surgery and another group using the same protocol 1 hour after surgery; the sample was composed of 24 patients with an average of 26 years and was evaluated on the 2nd, 5th and 7th day using the visual pain scale (VAS), they had a statistically significant difference as a result (p=0,008)in the group that used Dexamethasone before surgery when compared to the group that used 1 hour later regarding pain reduction. 20. This result reinforces the protocol used in this study to administer corticosteroids preoperatively.
Regarding edema, evaluated by means of quantitative observational analysis comparing visible asymmetry with the contralateral side, an effect of the moment was observed (Table 4, F(2,56)=141.96, p<0.001, ηp2=0.835), with an elevation on the third day and a tendency to decrease from the third to the seventh day and with similar behavior in both groups (stratified by corticoid used preoperatively) (F(1,28)=0,840, p 0.367, ηp2=0.029).
Regarding the differences in the routes of administration of corticosteroids, a randomized controlled trial conducted by Antunes et al.14 aimed to compare the efficacy of 8 mg dexamethasone administered by 2 different routes, oral versus intramuscular administration. The authors found no significant differences (p=0.128) between the route of drug administration in the reduction of edema using facial reference in the quantification of edema in a sample of 67 patients with an average age of 14 - 37 years and analyses performed on the 2nd and 7th postoperative day. In addition, participants who used Dexamethasone had better results in this regard than the control group who did not use corticosteroids preoperatively. In the same vein, Chaudary et al.15 compared the preventive effect of 4 mg of Dexamethasone intravenously versus an oral administration of 8 mg of Dexamethasone in 200 volunteers averaging 20 years of age with follow-up at 24 hours, 48 hours, and day 7 through analysis with measurement of the edema by standardizing measurement points on the face. They found that both routes of administration were equally effective in reducing postoperative edema (p=0.631). This is because an oral corticosteroid, such as Dexamethasone 8 mg, has a very high enteral absorption rate comparable to intravenous application. Thus, oral Dexamethasone is a good alternative to the intravenous or Intramuscular route in patients who do not wish to receive an injection 14, 15, 21. Silva19 also found no significant differences (p=0.874) when they compared Dexamethasone and Betamethasone, both 4mg orally, in an analysis on a postoperative day 3 in patients who removed third molars.
Regarding the maximum mouth opening, evaluated by measuring the distance between the incisal edges of the upper and lower central incisors, an effect of the moment was observed (Table 4, F(2,56)=141.96, p <0.001, ηp2=0.835), with a limitation of mouth opening on the third day and a tendency to normalize from the third to the seventh day and with similar behavior in both groups (stratified by corticoid used preoperatively) (F(1,28)=2.42, p 0.131, ηp2=0.080)19.conducted a study with 40 volunteers comparing the efficacy of Dexamethasone 4mg and betamethasone 4mg and, as in this study, quantified the maximum mouth opening by measuring the distance between the incisal edges of the upper and lower central incisors with a millimeter ruler at 24 hours, 72 hours, and on the seventh day postoperatively, and found no differences between the drug protocols on day 3 (p=0.631), as in this study. Another study compared the preventive effect of 4 mg dexamethasone intravenously against an oral administration of 8 mg dexamethasone in 200 volunteers aged 20 years on average with follow-up at 24 hours, 48 hours, and day 7, resulting in equivalent results regardless of the protocol used. (p=0.569)15.
Still, on mouth opening, a study using electromyography in the postoperative period found efficacy (p<0.05) in patients who used corticosteroids preoperatively (Dexamethasone and cyclobenzaprine) when compared to the control group (no prior medication), the study had a sample of 15 volunteers (30 lower third molars extracted) in patients aged 20 to 30 years, the examinations were performed in the immediate postoperative period and on the seventh day after surgery 7. This work also reinforces the design chosen in the present study regarding the timing of corticoid administration.
The main limitations of this study refer to the standardization of patient positioning since the alignment for thermal image collection was performed according to directional lines using a tape measure, and no fixed positioner was used. Regarding the standardization of the surgical procedure, even though the operation was performed in all patients in the study by the same surgeon, and the position was standardized, there are still differences in the transoperative period according to patient compliance, surgical time, consequently impacting on tissue trauma generated during manipulation. Besides the above, the patient's collaboration in postoperative care influences the evolution of the inflammatory process in an important way. Even with the explanation of the need for drug therapy in the postoperative, the results are dependent on the patient's collaboration to follow the guidelines given to them.
CONCLUSIONS
To the best of our knowledge, this study was the first to evaluate the signs of the inflammatory process by thermal imaging in the postoperative period of impacted and semi-impacted third molar extractions in patients who used an oral Dexamethasone or an intramuscular Betamethasone Dipropionate + Betamethasone Disodium Phosphate drug protocol. It can be concluded that there is an effect of the interaction moment of assessment + corticoid on the absolute temperatures of the ROI of the mandibular angle during the postoperative period of patients submitted to surgery for extraction of impacted and semi-impacted third molars using different preoperative drug protocols.
Betamethasone dipropionate + betamethasone disodium phosphate (5mg/mL + 2mg/mL) in injectable form showed inferior performance in controlling the increase in skin temperature, which is one of the cardinal signs of inflammation in the facial region when compared to Dexamethasone orally (8mg).
Regarding pain sensitivity, edema, and mouth opening, although an effect of the moment of the evaluation was observed in the measured values, there was no significant difference according to the drug protocol used. Therefore, considering the results of this study, we recommend the use of oral Dexamethasone 8.0 mg (02 tablets of 4.0 mg) one hour before surgical procedures for removal of impacted and semi-impacted third molars in order to control the inflammatory response during the postoperative period, since its administration is less invasive and its action is satisfactory.
Author Contributions: Conceptualization, JN and EN; methodology, JN, EN and DH; validation, JN, EN and DH; formal analysis, EN and DH; investigation, JH and BM; resources, EN, LU; data curation, JN; writing—original draft preparation, JN; writing—review and editing, EN; visualization, LU and AZ; supervision, EB, DH and AZ; project administration, EN and DH; funding acquisition, YY All authors have read and agreed to the published version of the manuscript.
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study (the project was registered and approved at Plataforma Brasil under number CAAE 48596621.0.0000.5547).
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. Larsen, M.K.; Kofod, T.; Christiansen, A.E.; Starch-Jensen, T. Different Dosages of Corticosteroid and Routes of Administration in Mandibular Third Molar Surgery: a Systematic Review. J Oral Maxillofac Res. 2018,9,22.
2. Kasprzyk-Kucewicz, T.; Cholewka, A.; Bałamut, K.; Kownacki, P.; Kaszuba, N.; Kaszuba, M.; Morawiec, T. Aplicações da termografia infravermelha na remoção cirúrgica de dentes retidos avaliação dos efeitos. Journal of Thermal Analysis and Calorimetry. 2021,144,139-144.
3. Xu, J.L.; Xia, R. Influence factors of dental anxiety in patients with impacted third molar extractions and its correlation with postoperative pain: a prospective study. Med Oral Patol Oral Cir Bucal. 2020,1,25.
4. Braimah, R. O.; Ibikunle, A. A.; Taiwo, A. O. Ndukwe, K. C.; Owotade, J. F.; Aregbesola, S. B. Pathologies associated with impacted mandibular third molars in Sub-Saharan Africans. Dent Med Res. 2018,6,41.
5. Garbin, C. A. S.; Garbin, A. J. I.; Rovida, T. A. S.; Moroso, T. T.; Dossi, A. P. Conhecimento sobre prescrição medicamentosa entre alunos de Odontologia: o que sabem os futuros profissionais? Rev Odontol UNESP. 2020,36,323-9.
6. Ngeow, W.C.; Lim, D. Do Corticosteroids Still Have a Role in the Management of Third Molar Surgery? Adv Ther. 2016;33,1105.
7. Raldi, Veo. Avaliação do impacto do uso pré-operatório de dexametasona e ciclobenzaprina em exodontias cirúrgicas de terceiros molares inferiores em trismo por análise eletromiográfica. Cirurgia Oral e Maxilofacial. 2019,2,395.
8. Rabelo, R.; Gomes, A. Corticosteróides e anti-inflamatórios não esteróides em cirurgia oral: indicação de uso. Pesquisa, Sociedade e Desenvolvimento. 2022,1,26.
9. Gerino, J.; Neto, E.; Ferreira, L.; Cangusu, M.; Sardinha, S.; Cavalcante, W. Uso de corticoides por cirurgiões bucomaxilofaciais do Brasil. Revista de Ciências da Saúde e Biológicas. 2020,1,33.
10. Haddad, D. S.; Brioschi, M. L.; Luchetti, M. A. B.; Civiero, N.; Moreira, M. A.; Arita, E. S. Thermographic Toothache Screening by Artificial Intelligence. In MICCAI Workshop on Medical Image Assisted Blomarkers' Discovery. Cham: Springer Nature Switzerland. 2022, 1,45-56.
11. Aires, M.M. Fisiologia. 5 ed: Guanabara; 2018.
12. Ventä, I.; Hyrkäs, T.; Paakkari, I.; Ylipaavalniemi, P. Thermographic imaging of postoperative inflammation modified by anti-inflammatory pretreatment. J Oral Maxillofac Surg. 2001,2,145.
13. Boonsiriseth, K.; Klongnoi, B.; Sirintawat, N.; Saengsirinavin, C.; Wongsirichat, N. Comparative study of the effect of dexamethasone injection and consumption in lower third molar surgery. Int J Oral Maxillofac Surg. 2012,2,244.
14. Antunes, A.A.; Avelar, R.L.; Martins Neto, E.C.; Frota, R.; Dias, E. Effect of two routes of administration of Dexamethasone on pain, edema, and trismus in impacted lower third molar surgery. Oral Maxillofac Surg. 2011,4,217.
15. Chaudhary, P.D.; Rastogi, S.; Gupta, P.; Niranjanaprasad Indra, B.; Thomas, R.; Choudhury, R. Pre-emptive effect of dexamethasone injection and consumption on postoperative swelling, pain, and trismus after third molar surgery. A prospective, double blind and randomized study. J Oral Biol Craniofac Res. 2015;5,21.
16. Sousa, R. Beclonato, medicamento similar. Laboratório Ducto Indústria Farmacêutica LTDA.2011.
17. Bertollo, A.; Demartini, C.; Piato, A.L. Interações Medicamentosas na Clínica Odontológica. Revista Brasileira de Odontologia. 2013,70,120.
18. Cruz PC, A. Corticosteroides injetáveis em patologia músculo-esquelética: Uma revisão Narrativa. Revista da SPMFR. 2021,33,74.
19. Silva, M. Ensaio clínico randomizado triplo cego utilizando dois diferentes protocolos para controle de dor, trismo e edema após exodontia de terceiros molares inferiores. Mossoró: Universidade do Estado do Rio Grande do Norte; 2020.
20. Al-Shamiri, H.M.; Shawky, M.; Hassanein, N. Comparative Assessment of Preoperative versus Postoperative Dexamethasone on Postoperative Complications following Lower Third Molar Surgical Extraction. Int J Dent. 2017, 350375.
21. Bortoluzzi, M.; Capela, D.; Barbieri, T.; Plagiarini, M.; Cavaleiro, T.; Manfro, R. A single dose of amoxicillin and Dexamethasone for the prevention of postoperative complications in third molar surgery: a randomized, double-blind, placebo-controlled clinical trial. J Clin Med Res. 2013,5,26.
Received: March 1, 2024 / Accepted: July 17, 2024 / Published: September 15, 2024.
Citation: Hálice Noronha J, Sabbagh Haddad D, Ulbricht L, Martini B, Zetola A L, Borba Neves E. Clinical and Thermographic Evaluation of the Inflammatory Response to Third Molar Removal. Bionatura Journal 2024; 1 (3) 21. http://dx.doi.org/10.70099/BJ/2024.01.03.21
Additional information
ISSN 3020-7886
Correspondence should be addressed to noronhajessicahalice@gmail.com
Peer review information. Bionatura Journal thanks the anonymous reviewers for their contribution to the peer review of this paper using https://reviewerlocator.webofscience.com/.
All articles published by Bionatura Journal are freely and permanently accessible online immediately upon publication, with no subscription fees or registration barriers.
Editor's note: Bionatura Journal remains neutral regarding jurisdictional claims in published maps and institutional affiliations.
Copyright: © 2024 by the authors. Submitted for possible open-access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).