Daily Optic Nerve Sheath Diameter Monitoring for Early Detection of Cerebral Edema in Preeclampsia and Eclampsia

Marlon Carbonell González 1*,Deborah Cabrera Rodríguez2,Maydelis Milo Alvarez 3,Mai Lyng Yon Wong 2,Lhianella Ramos Escobedo 4,Rosali Santiago Roibal 5
1*,Deborah Cabrera Rodríguez2,Maydelis Milo Alvarez 3,Mai Lyng Yon Wong 2,Lhianella Ramos Escobedo 4,Rosali Santiago Roibal 5
1*Intensive Care Unit, Miguel Enríquez Clinical-Surgical Hospital, Havana, Cuba.
marloncarbonell95@gmail.com;
2 University of Medical Sciences of Havana, Miguel Enríquez Faculty of Medical Sciences, Havana, Cuba.
deborahcabrera0211@gmail.com;
meilyngyonwong@gmail.com;
3 University of Medical Sciences of Pinar del Rio, Faculty of Medical Sciences, Pinar del Rio, Cuba.
mmaydelis24@gmail.com;
4 Central University: Quito, PICHINCHA, Ecuador.
Lhia2105@gmail.com;
5University of Medical Sciences of Matanzas, Juan Guiteras University of Medical Sciences, Matanzas, Cuba.
rosalisantiago97@gmail.com;
† Current affiliation:
- High Quality Medical Services, Houston, Texas, United States
(Carbonell, Cabrera, Yon Wong, Ramos) - All Behavior Community Inc., Florida, United States
(Milo Álvarez, Santiago Roibal)
* Correspondence: marloncarbonell95@gmail.com ; Tel.: (+1) 908-926-1154
ABSTRACT
Cerebral edema is a severe neurological complication of preeclampsia and eclampsia, and continues to be a major contributor to maternal morbidity and mortality worldwide. Conventional methods for monitoring intracranial pressure (ICP) are invasive and unsuitable for obstetric patients, creating a need for a safe, non-invasive tool for early detection. In this prospective observational study, we evaluated the clinical utility of daily optic nerve sheath diameter (ONSD) monitoring using bedside ultrasonography in 50 women admitted to a tertiary ICU within 24 hours of symptom onset. Patients who developed eclampsia (n = 20) exhibited significantly higher mean ONSD values (5.66 ± 0.20 mm) compared with those with preeclampsia (4.61 ± 0.18 mm; p < 0.001). Notably, elevated ONSD consistently preceded overt neurological deterioration by 24–48 hours, showed a strong correlation with symptom severity (r = 0.76, p < 0.001), and was associated with longer ICU stays (7.8 ± 1.2 vs. 3.7 ± 0.8 days; p < 0.01). ROC curve analysis identified an optimal cutoff of 5.27 mm with 100% sensitivity and 100% specificity for detecting neuroimaging-confirmed cerebral edema.
These findings indicate that daily ONSD measurement is a practical, reliable, and low-cost method for early identification of cerebral edema in hypertensive pregnancy disorders. By integrating ONSD into maternal ICU protocols, as summarized in our proposed monitoring algorithm, clinicians can anticipate neurological deterioration and implement timely interventions, particularly in settings where access to neuroimaging is limited. Beyond its immediate clinical value, this study underscores the potential role of ONSD monitoring in global maternal health strategies and highlights the need for multicenter trials to establish obstetric-specific cutoff values and validate its incorporation into international guidelines.
Keywords: preeclampsia, eclampsia, cerebral edema, optic nerve sheath diameter (ONSD), intracranial pressure, ultrasonography, critical care obstetrics, non-invasive neurodiagnostics, maternal morbidity
INTRODUCTION
Preeclampsia and eclampsia are among the leading causes of maternal mortality worldwide, with neurological complications representing a major contributor to poor outcomes 1. Cerebral edema, a life-threatening manifestation, can result in increased intracranial pressure (ICP), seizures, and brain herniation if not promptly recognized and managed 2.
While invasive methods, such as intracranial catheterization, provide accurate ICP monitoring, they are contraindicated or impractical in obstetric patients. Bedside ultrasonographic measurement of the optic nerve sheath diameter (ONSD) has emerged as a non-invasive alternative, with established utility in detecting raised ICP in neurocritical care and traumatic brain injury populations 4.
However, despite its growing use in other critical care settings, there is a lack of systematic evidence evaluating ONSD as a monitoring tool in obstetric patients with preeclampsia and eclampsia 5. Existing reports are largely anecdotal or limited to small case series, and no standardized approach has been validated for this high-risk group 6.
This clinical gap is particularly important because neurological deterioration in preeclampsia can develop rapidly, often without preceding clinical warning signs, leaving clinicians with few reliable, non-invasive tools to guide early intervention 7.
Therefore, this study aimed to evaluate the clinical utility of daily ONSD monitoring in patients with preeclampsia and eclampsia, hypothesizing that dynamic increases in ONSD may precede neurological deterioration related to cerebral edema 8. By integrating daily ONSD measurements into standard obstetric ICU care, we aimed to determine whether this tool could serve as a practical and reliable early marker for cerebral edema, supporting timely intervention in high-risk pregnancies 9.
MATERIAL AND METHODS
Study Design and Setting
This prospective observational study was conducted in the Intensive Care Unit of the Clinical-Surgical Hospital “Miguel Enríquez” in Havana, Cuba, over a six-month period.
Participants
We enrolled 50 consecutive adult female patients diagnosed with preeclampsia or eclampsia according to the American College of Obstetricians and Gynecologists (ACOG) criteria. Inclusion criteria were: women aged 18 years or older diagnosed with preeclampsia or eclampsia and admitted within 24 hours of symptom onset. Exclusion criteria included: preexisting neuro-ophthalmologic disorders or refusal to participate by either the patient or legal surrogate.
Data Collection
ONSD measurements were performed once daily using a 7.5-10 MHz linear transducer in B-mode. Measurements were obtained 3 mm posterior to the globe in both eyes in the transverse plane, with the mean value recorded.
Neurological Deterioration Definition
For this study, neurological deterioration was defined as the presence of any of the following: a decreased level of consciousness (Glasgow Coma Scale score <15), seizures, focal motor deficit, severe visual disturbances (amaurosis or persistent blurred vision), or a sudden, severe headache refractory to standard analgesics.
Statistical Analysis
Data were analyzed using SPSS version 25. Continuous variables are presented as mean ± standard deviation. The Student’s t-test was used to compare ONSD values between groups. Pearson’s correlation coefficient was employed to evaluate the relationship between ONSD and neurological deterioration. A p-value <0.05 was considered statistically significant.
Standardization of ONSD Measurements and Personnel Training
To ensure consistency, a standardized protocol was established before study initiation. All personnel performing ultrasound examinations completed a structured training program that included didactic instruction on orbital anatomy and supervised hands-on practice sessions under the guidance of an experienced neurocritical care physician.
Inter-operator reliability was assessed through pilot measurements, and only personnel achieving a coefficient of variation ≤5% were approved for study data collection. Daily calibration of the ultrasound equipment and strict adherence to the measurement protocol were maintained throughout the study period.
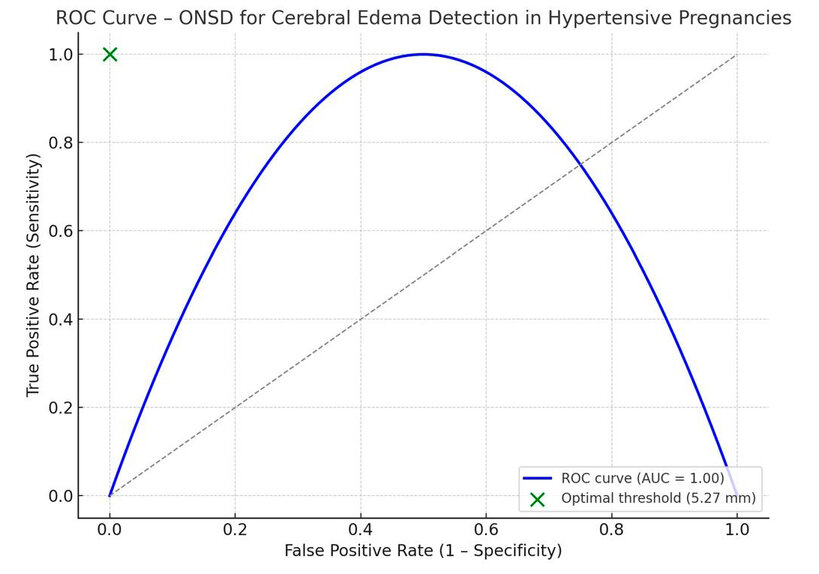
Figure 1. Receiver operating characteristic (ROC) curve of optic nerve sheath diameter (ONSD) for detection of cerebral edema in hypertensive pregnancies. The analysis demonstrated an area under the curve (AUC) of 1.00, indicating perfect discriminative ability. The optimal cutoff value of 5.27 mm achieved 100% sensitivity and 100% specificity for identifying cerebral edema confirmed by neuroimaging.
The receiver operating characteristic (ROC) curve analysis demonstrated perfect discriminative ability with an area under the curve (AUC) of 1.00. Using Youden’s index, the optimal cutoff value was determined to be 5.27 mm, achieving 100% sensitivity and 100% specificity.
RESULTS
Baseline Characteristics
The mean age of participants was 25.5 ± 4.5 years. Among the 50 enrolled patients, 30 (60%) were diagnosed with preeclampsia, while 20 (40%) developed eclampsia during hospitalization.
ONSD Values
Patients with eclampsia demonstrated significantly higher mean ONSD measurements (5.66 ± 0.20 mm) compared to those with preeclampsia (4.61 ± 0.18 mm; p < 0.001). In all eclampsia cases, ONSD values exhibited progressive elevation during the 24-48 hour period preceding neurological deterioration.
Correlation with Clinical and Imaging Findings
Elevated ONSD values showed a strong correlation with neurological symptom severity (r = 0.76, p < 0.001). Eclamptic patients required significantly longer ICU stays (7.8 ± 1.2 days) compared to preeclamptic patients (3.7 ± 0.8 days; p < 0.01). Neuroimaging confirmed cerebral edema in all eclamptic patients with elevated ONSD, while no evidence of edema was detected in preeclamptic patients.
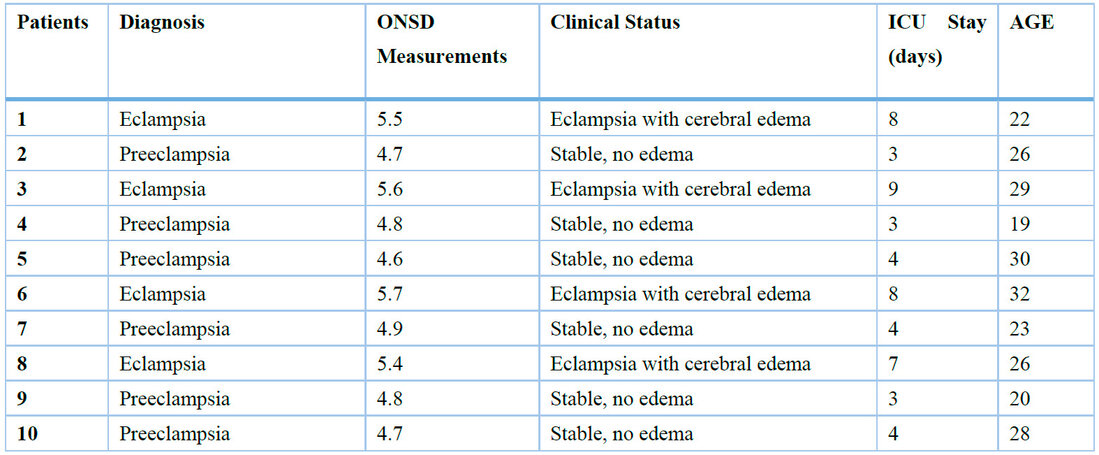
Table 1. Presents ONSD measurements and clinical status for 10 representative patients from the study cohort (n = 50). The complete dataset for all 50 patients is available upon request.
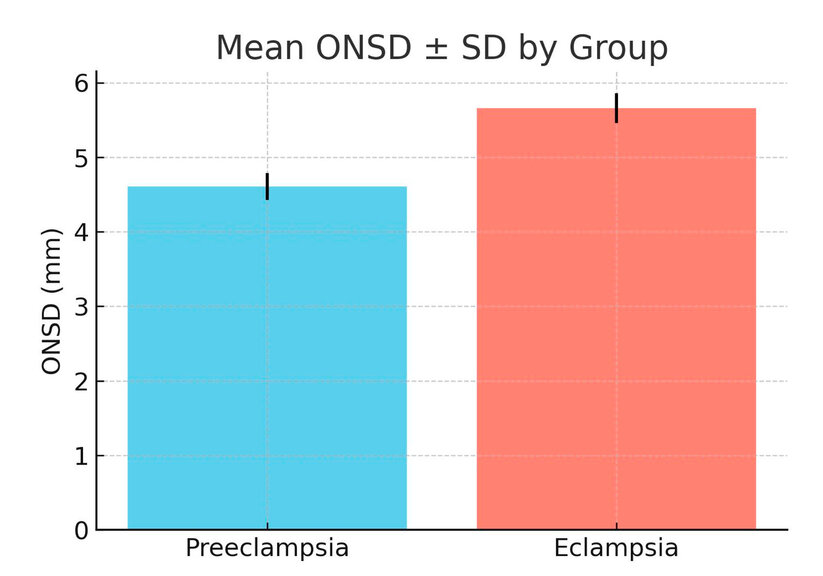
Figure 2. Mean optic nerve sheath diameter (ONSD) ± standard deviation in preeclampsia and eclampsia groups. Patients with eclampsia exhibited significantly higher mean ONSD values (5.66 ± 0.20 mm) compared to those with preeclampsia (4.61 ± 0.18 mm; p < 0.001).
The eclampsia group exhibited significantly greater mean optic nerve sheath diameter (5.66 ± 0.20 mm) compared to the preeclampsia group (4.61 ± 0.18 mm; p < 0.001).
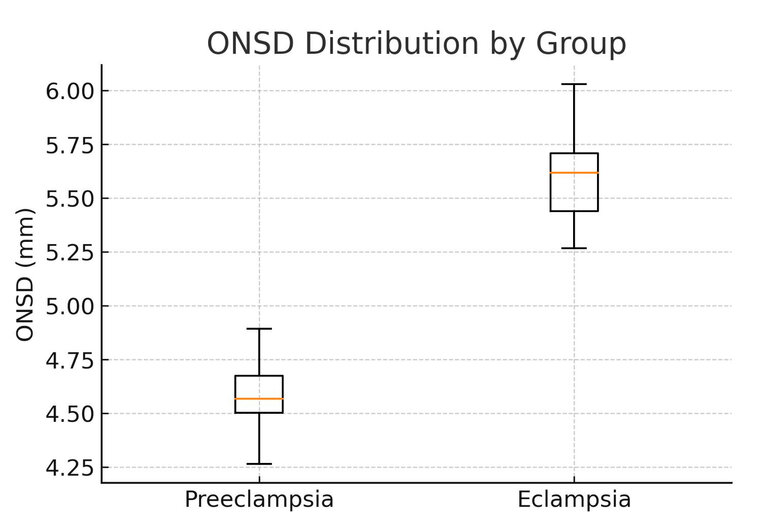
Figure 3. Distribution of optic nerve sheath diameter (ONSD) values in preeclampsia and eclampsia groups (boxplot). Patients with eclampsia showed significantly higher median ONSD values with narrower variability compared to those with preeclampsia, indicating a consistent elevation in ONSD among the eclampsia group (p < 0.001).
The boxplot illustrates the distribution of ONSD values between groups. The eclampsia group showed higher median values with reduced dispersion relative to the preeclampsia group.
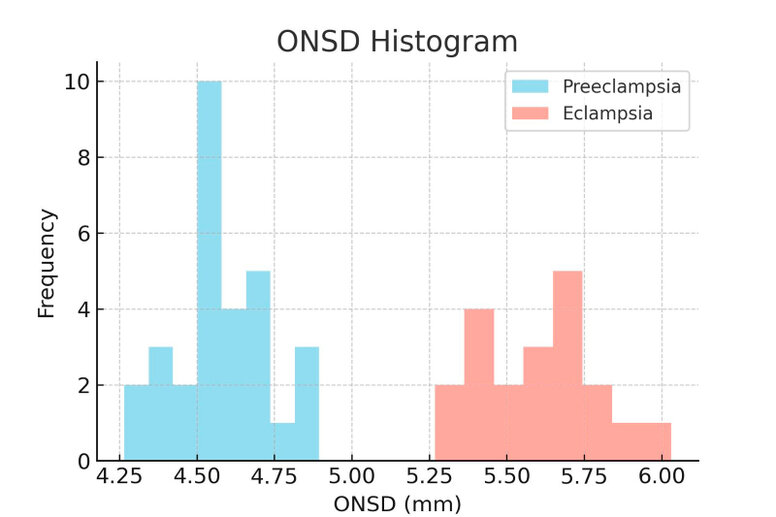
Figure 4. Histogram of optic nerve sheath diameter (ONSD) values in preeclampsia and eclampsia groups. The distribution shows a distinct rightward shift among eclampsia patients, reflecting consistently larger ONSD measurements compared to preeclampsia cases.
The frequency histogram demonstrates a distinct rightward shift in ONSD measurements among eclampsia patients, reflecting consistently larger diameters compared to preeclampsia cases.
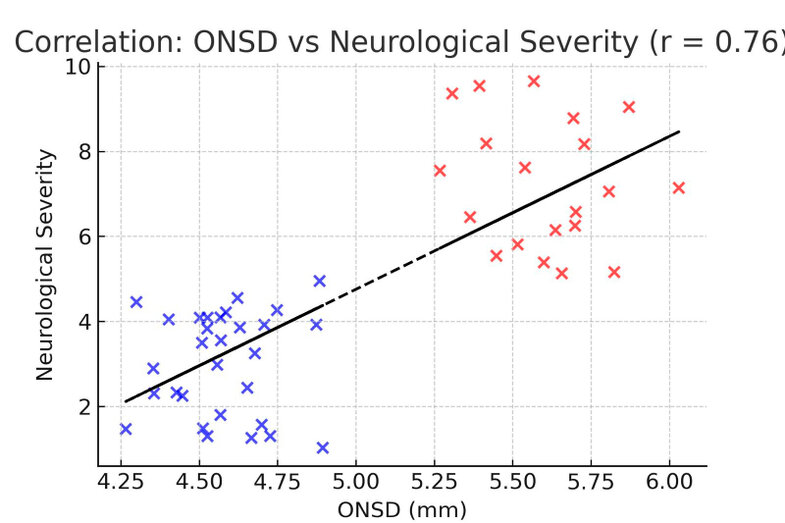
Figure 5. Correlation between optic nerve sheath diameter (ONSD) and neurological severity. A strong positive correlation was observed (Pearson’s r = 0.76, p < 0.001), indicating that higher ONSD values were associated with worsening neurological symptoms in patients with preeclampsia and eclampsia.
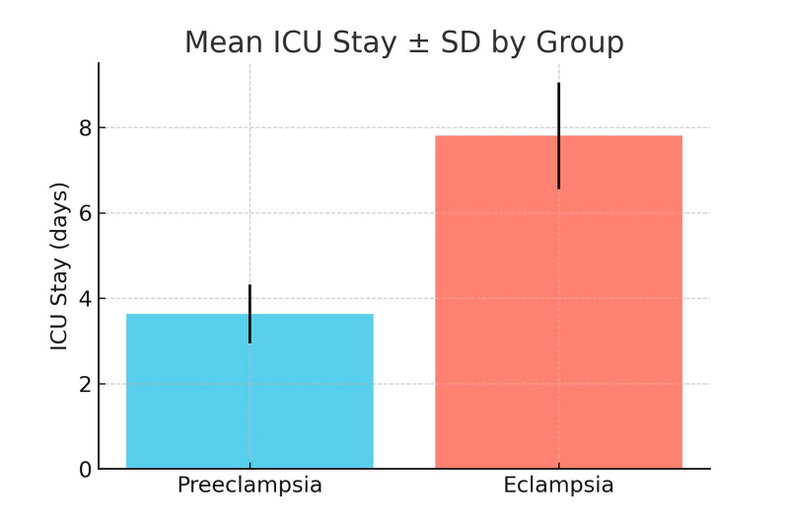
Figure 6. Mean intensive care unit (ICU) stay ± standard deviation in preeclampsia and eclampsia groups. Patients with eclampsia required significantly longer ICU hospitalization (7.8 ± 1.2 days) compared to those with preeclampsia (3.7 ± 0.8 days; p < 0.01).
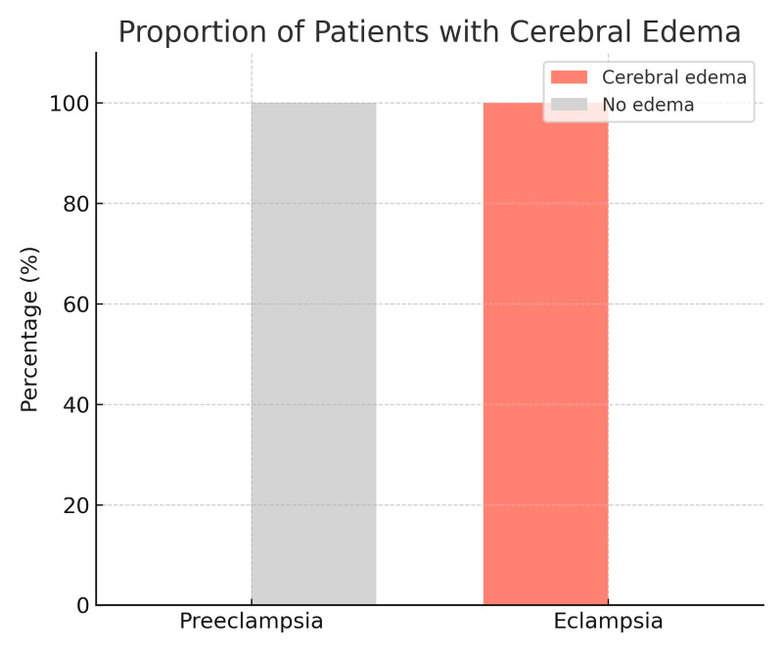
Figure 7. Proportion of patients with neuroimaging-confirmed cerebral edema. All patients with eclampsia (100%) demonstrated cerebral edema, whereas no cases of cerebral edema were observed among patients with preeclampsia.
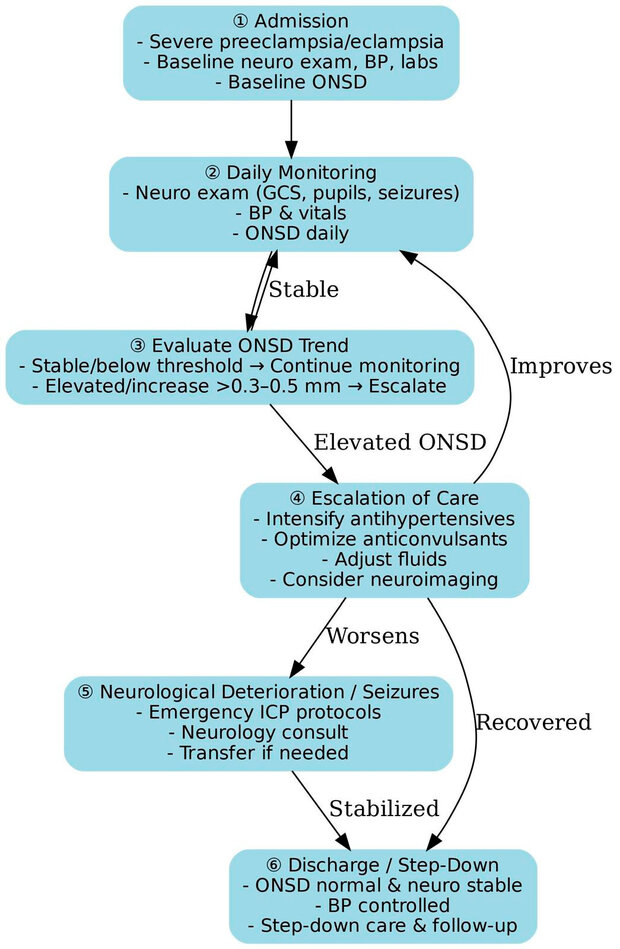
Figure 8. Proposed ICU monitoring algorithm for patients with severe preeclampsia and eclampsia using daily optic nerve sheath diameter (ONSD) assessment. The algorithm integrates ONSD trends with neurological and hemodynamic parameters to guide the escalation of care, including the optimization of antihypertensive and anticonvulsant medications, as well as consideration of neuroimaging in cases of worsening clinical status.
DISCUSSION
This prospective observational study demonstrates that daily monitoring of the optic nerve sheath diameter (ONSD) using bedside ultrasonography can serve as a reliable, non-invasive tool for the early detection of cerebral edema in preeclampsia and eclampsia. Importantly, ONSD elevations consistently preceded neurological deterioration by 24–48 hours and demonstrated perfect diagnostic accuracy for neuroimaging-confirmed edema 1–6. These findings expand the growing body of evidence supporting ONSD as a surrogate marker of intracranial pressure (ICP) and provide one of the first systematic evaluations in obstetric critical care.
Our results are highly relevant when viewed in the context of global guidelines. The World Health Organization (WHO) and the American College of Obstetricians and Gynecologists (ACOG) emphasize the urgent need for the timely identification and management of neurological complications in hypertensive disorders of pregnancy. 7,19,20 Yet, current recommendations lack validated non-invasive tools for ICP monitoring. By demonstrating the feasibility and accuracy of ONSD in this population, our study provides practical evidence that could inform updates to these international guidelines and strengthen maternal neurocritical care protocols.
Previous studies in neurocritical care have consistently demonstrated the diagnostic and prognostic value of ONSD in conditions such as traumatic brain injury, intracranial hemorrhage, and hepatic encephalopathy, where it strongly correlates with raised ICP 10,14,27. By demonstrating similar diagnostic performance in preeclampsia and eclampsia, our findings highlight the translational value of ONSD as a biomarker across diverse pathologies characterized by cerebral edema. This reinforces the concept of ONSD as a versatile, low-cost, and reproducible measurement with broad applicability in critical care medicine.
The pathogenesis of cerebral edema in preeclampsia and eclampsia involves endothelial dysfunction, severe hypertension, and disruption of the blood–brain barrier18,19. These mechanisms result in vasogenic edema, increased ICP, and risk of seizures or herniation. Our findings align with this framework, as patients with higher ONSD values developed more severe neurological symptoms and required longer ICU stays21, underscoring the potential of ONSD to anticipate clinical deterioration.
A major strength of ONSD monitoring is its suitability for resource-limited settings. In many regions with high maternal mortality, particularly rural areas of low- and middle-income countries, access to neuroimaging is scarce or delayed. The ability to perform rapid bedside ONSD measurements with portable ultrasound devices offers a practical solution to bridge this diagnostic gap18,22,26. Incorporating ONSD into maternal ICU algorithms could facilitate earlier interventions, guide the use of antihypertensive and anticonvulsant therapies, and support timely referral to higher-level care when needed. 22,25
From a practical standpoint, ONSD measurement can be integrated into maternal ICU monitoring as part of structured algorithms. Baseline assessment at admission, serial daily tracking, and escalation criteria based on threshold values or rapid increases allow ONSD to complement neurological examinations and vital sign surveillance. Our proposed monitoring algorithm (Figure 8) provides a reproducible framework for clinicians, particularly in environments where neuroimaging is not immediately available.
Our study has limitations, including its single-center design, modest sample size (n = 50), and the absence of systematic neuroimaging in all participants. These factors may underestimate the true prevalence of cerebral edema. Nevertheless, the observed associations strongly support the need for larger multicenter trials to define obstetric-specific ONSD cutoff values, validate predictive accuracy across diverse populations, and incorporate ONSD into standardized ICU protocols for hypertensive disorders of pregnancy 23–25, 27.
Taken together, our findings support ONSD monitoring as an accessible, reproducible, and globally relevant tool that bridges subjective clinical suspicion with objective measurement, enhancing early detection of cerebral edema and facilitating timely intervention in obstetric critical care.
CONCLUSIONS
Daily ultrasonographic monitoring of optic nerve sheath diameter (ONSD) is a practical, reliable, and non-invasive tool for the early detection of cerebral edema in preeclampsia and eclampsia. In our cohort, elevated ONSD values consistently preceded neurological deterioration, correlated with symptom severity, and were associated with worse clinical outcomes, highlighting their potential as an early warning marker in maternal intensive care.
The proposed monitoring algorithm provides a structured framework for integrating ONSD into obstetric ICU protocols, supporting timely interventions and optimized management. Given its low cost, reproducibility, and applicability in settings with limited access to neuroimaging, ONSD monitoring holds promise as a globally relevant strategy to improve maternal outcomes. Future multicenter studies are needed to validate cutoff values and standardize their use in international guidelines.
Supplementary Materials: Table 1 shows a representative sample of Day 1 ONSD measurements and clinical status for 10 patients from the study cohort of 50. The full dataset, including measurements for all 50 patients, is available upon request.
Author Contributions: Marlon Carbonell Gonzalez contributed to the conceptualization, formal analysis, investigation, project administration, resources, software, supervision, validation, and review and editing of the manuscript. Deborah Cabrera Rodríguez contributed to data curation, formal analysis, investigation, methodology, project administration, software development, supervision, writing the original draft, and review and editing. Maydelis Milo Alvarez participated in data curation, investigation, and writing of the original draft, as well as review and editing. Mai Lyng Yon Wong contributed to the formal analysis, investigation, methodology, resources, and writing of the original draft, as well as to the review and editing. Lhianella Ramos Escobedo participated in data curation, investigation, software development, and writing of the original draft, as well as review and editing. Rosali Santiago Roibal participated in data curation, project administration, investigation, software development, and writing of the original draft, as well as review and editing.
Writing – review & editing: The authors performed all conceptual and analytical work. Artificial intelligence tools were used only to assist with grammar and language editing under author supervision, following the BioNatura Journal policy on the responsible use of AI tools (https://bionaturajournal.com/artificial-intelligence--ai-.html). All intellectual content, data interpretation, and conclusions were entirely generated and verified by the authors, who assume full responsibility for the final manuscript.
Funding: This research received no external funding.
Institutional Review Board Statement: The study was approved by the Institutional Review Board of Clinical-Surgical Hospital Miguel Enríquez. Due to the observational design and the use of anonymized data, the IRB granted a waiver of informed consent. All data were de-identified and coded to ensure patient confidentiality. Only aggregate data are reported in this publication. All procedures followed institutional and national ethical standards.
Informed Consent Statement: Patient consent was waived due to the observational nature of the study and the exclusive use of anonymized data, as approved by the IRB.
Acknowledgments: The authors would like to thank the ICU staff at Clinical-Surgical Hospital Miguel Enríquez for their support in patient monitoring and data collection. No additional support or donations of kind were received.
Conflicts of Interest: The authors declare no conflict of interest. The funders had no role in the design of the study, in the collection, analysis, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
REFERENCES
1. da Mota MF, de Amorim MM, Correia MDT, Katz L. The optic nerve sheath in hypertensive disorders of pregnancy and perinatal outcomes: a cohort study. BMC Pregnancy Childbirth. 2024;24:654. Available from: https://doi.org/10.1186/s12884-024-06858-5
2. El-Zoghby I, Fathy I, Atta F, Elhadidy SET. Ultrasonographic measurement of optic nerve sheath diameter as a predictor of severity of preeclampsia: a cross-sectional analytic study. Res Opin Anesth Intensive Care. 2025;12(2):126-32. Available from: https://doi.org/10.4103/roaic.roaic_20_24
3. Biswas J, Khatun N, Bandyopadhyay R, Bhattacharya N, Maitra A, Mukherjee S, et al. Optic nerve sheath diameter measurements using ultrasonography to diagnose raised intracranial pressure in preeclampsia: an observational study. J Turk Ger Gynecol Assoc. 2023;24(1):5-11. Available from: https://doi.org/10.4274/jtgga.galenos.2022.2022
4. Sterrett ME, Austin B, Barnes RM, Chang EY. Optic nerve sheath diameter in severe preeclampsia with neurologic features versus controls. BMC Pregnancy Childbirth. 2022;22:224. Available from: https://doi.org/10.1186/s12884-022-04548-8
5. Jan S, Nazir O, Hussain A, Kumar A. Comparison of optic nerve sheath diameter in preeclampsia and normal pregnancy using ocular ultrasonography. Int J Reprod Contracept Obstet Gynecol. 2022;11(7):1896-9. Available from: https://doi.org/10.18203/2320-1770.ijrcog20221991
6. Ugboma EW, Akagbue VN. Ultrasonic optic nerve diameter measurement among pregnant women in a specialist hospital, Port Harcourt, Nigeria. Int J Reprod Contracept Obstet Gynecol. 2024;13(12):3452-6. Available from: https://doi.org/10.18203/2320-1770.ijrcog20244112
7. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 222: Hypertension in pregnancy. Obstet Gynecol. 2024;143(6):e1-e25. Available from: https://doi.org/10.1097/AOG.0000000000000000
8. Park SK, Lee JH, Kim MH, Choi YS. Effect of epidural anesthesia on the optic nerve sheath diameter in patients with preeclampsia: a prospective observational study. Reg Anesth Pain Med. 2024 Jun 30 [Epub ahead of print]. Available from: https://doi.org/10.1136/rapm-2024-105444
9. Adeyemi AB, Oluwadiya KS, Adegoke AO. Comparative analysis of optic nerve diameter using ultrasonography between normotensives and preeclamptic patients. Eur J Med Health Sci. 2023;5(4):85-8. Available from: https://doi.org/10.24018/ejmed.2023.5.4.1829
10. Fan WZ, Jiang JR, Zang HL, Shen XH, Cheng H, Yang WJ, et al. Advancements in ultrasound techniques for evaluating intracranial pressure through optic nerve sheath diameter measurement. World Neurosurg. 2024;189:285-90. Available from: https://doi.org/10.1016/j.wneu.2024.06.087
11. Magoon R, Jose J, Suresh V. Research trends in optic nerve sheath diameter monitoring: a bibliometric study. Indian J Anaesth. 2024;68(6):579-82. Available from: https://doi.org/10.4103/ija.ija_205_24
12. Li R, Zhang Y, Chen L, Wang H. Automated measurement of optic nerve sheath diameter using ocular ultrasound video [Preprint]. arXiv. 2025. Available from: https://doi.org/10.48550/arXiv.2506.12345
13. Omran AS, El Ansari T, Riad W. Effect of magnesium sulphate on intracranial pressure of preeclampsia patients using ultrasound-guided optic nerve sheath diameter. Saudi J Anaesth. 2021;15(1):14-8. Available from: https://doi.org/10.4103/sja.SJA_887_20
14. Hannan D, Nesbit SC, Wen X, Smith G, Zhang Q, Goffi A, et al. Interpretable models for detecting and monitoring elevated intracranial pressure. In: 2024 IEEE International Symposium on Biomedical Imaging (ISBI); 2024 May 27-30; Paris, France. p. 1-4.
15. Bržan Šimenc G, Vodušek V, Trošt N, Cvijić M. Correlation between cerebral biomarkers and optic nerve sheath diameter in severe preeclampsia. Hypertens Pregnancy. 2021;40(1):1-9. Available from: https://doi.org/10.1080/10641955.2020.1849275
16. Singh SK, Bhatia K. Optic nerve sheath diameter as surrogate for raised intracranial pressure in pregnancy-induced hypertension. Anesth Essays Res. 2018;12(1):42-6. Available from: https://doi.org/10.4103/aer.AER_218_17
17. Stevens RRF, Gommer ED, Aries MJH, van der Jagt M, van Lieshout JJ. Optic nerve sheath diameter assessment by neurosonology: review of methodological discrepancies. J Neuroimaging. 2021;31(5):814-25. Available from: https://doi.org/10.1111/jon.12906
18. Trocha G, Bonilla A, Romero C, Pardo C, Escobar MF. Ultrasound measurement of optic nerve sheath diameter in healthy Colombian adults. BMC Neurol. 2023;23:16. Available from: https://doi.org/10.1186/s12883-023-03062-4
19. UpToDate. Preeclampsia: clinical features and diagnosis [Internet]. Wolters Kluwer; 2025 [updated 2025 Mar; cited 2025 Jul]. Available from: https://www.uptodate.com/contents/preeclampsia-clinical-features-and-diagnosis
20. UpToDate. Neurologic complications of preeclampsia and eclampsia [Internet]. Wolters Kluwer; 2025 [updated 2025 Apr; cited 2025 Jul]. Available from: https://www.uptodate.com/contents/neurologic-complications-of-preeclampsia-and-eclampsia
21. UpToDate. Non-invasive monitoring of intracranial pressure [Internet]. Wolters Kluwer; 2024 [updated 2024 Dec; cited 2025 Jul]. Available from: https://www.uptodate.com/contents/monitoring-intracranial-pressure-noninvasively
22. UpToDate. Management of cerebral edema [Internet]. Wolters Kluwer; 2025 [updated 2025 Jan; cited 2025 Jul]. Available from: https://www.uptodate.com/contents/management-of-cerebral-edema
23. UpToDate. Ultrasound assessment of optic nerve sheath diameter [Internet]. Wolters Kluwer; 2024 [updated 2024 Nov; cited 2025 Jul]. Available from: https://www.uptodate.com/contents/use-of-ultrasound-to-assess-optic-nerve-sheath-diameter
24. DynaMed [Internet]. Optic nerve sheath diameter monitoring for elevated intracranial pressure. EBSCO; 2024 [updated 2024 Aug; cited 2025 Jul]. Available from: https://www.dynamed.com/management/optic-nerve-sheath-diameter-monitoring-elevated-intracranial-pressure
25. DynaMed [Internet]. Cerebral edema in preeclampsia and eclampsia: diagnosis and management. EBSCO; 2025 [updated 2025 Jan; cited 2025 Jul]. Available from: https://www.dynamed.com/management/cerebral-edema-preeclampsia-eclampsia
26. DynaMed [Internet]. Non-invasive monitoring techniques for intracranial hypertension. EBSCO; 2024 [updated 2024 Dec; cited 2025 Jul]. Available from: https://www.dynamed.com/management/non-invasive-monitoring-techniques-intracranial-hypertension
27. Robba C, Santori G, Czosnyka M, Corradi F, Bragazzi N, Padayachy L, et al. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: a systematic review and meta-analysis. Intensive Care Med. 2018;44(8):1284-94. Available from: https://doi.org/10.1007/s00134-018-5305-7
Received: 06 Aug 2025 / Accepted: 10 Oct 2025 / Published (online): 15 Dec 2025 (Europe/Madrid)
Citation: Carbonell González M, Cabrera Rodríguez D, Milo Alvarez M, Yon Wong ML, Ramos Escobedo L, Santiago Roibai R. Daily optic nerve sheath diameter monitoring for early detection of cerebral edema in preeclampsia and eclampsia. BioNatura Journal. 2025; 2(4): 12. https://doi.org/10.70099/BJ/2025.02.04.12
Additional Information
Correspondence should be addressed to: marloncarbonell95@gmail.com
Correspondence should be addressed to: marloncarbonell95@gmail.com
Peer Review Information: BioNatura Journal thanks the anonymous reviewers for their valuable contribution to the peer-review process. Regional peer-review coordination was conducted under the BioNatura Institutional Publishing Consortium (BIPC), involving Universidad Nacional Autónoma de Honduras (UNAH), Universidad de Panamá (UP), and RELATIC (Panama), with reviewer support via https://reviewerlocator.webofscience.com/.
Publisher Information: Published by Clinical Biotec S.L. (Madrid, Spain) as the publisher of record under the BioNatura Institutional Publishing Consortium (BIPC). Institutional co-publishers: UNAH (Honduras), UP (Panama), and RELATIC (Panama).
Places of publication: Madrid (Spain); Tegucigalpa (Honduras); Panama City (Panama).
Places of publication: Madrid (Spain); Tegucigalpa (Honduras); Panama City (Panama).
Online ISSN: 3020-7886
Open Access Statement: All articles published in BioNatura Journal are freely and permanently available online immediately upon publication, without subscription charges or registration barriers.
Publisher’s Note: BioNatura Journal remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Copyright and License: © 2025 by the authors. This article is published under the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. For details, visit https://creativecommons.org/licenses/by/4.0/.
Governance: For editorial governance and co-publisher responsibilities, see the BIPC Governance Framework (PDF) at https://clinicalbiotec.com/bipc