Broad-Spectrum Antibiotic Resistance in septic patients in an Ecuadorian Intensive Care Unit of the Hospital Provincial General Docente of Riobamba

Carlos Yepez 1*; Zully Romero 2; Lizeth Aldaz 3; Katerin Trujillo 4 ; Marco Almache5
1* Coordinator of the Teaching and Research/Investigation Unit (Hospital Provincial General Docente / Riobamba / Ecuador); med.carlos.andres@gmail.com ;
2 Coordinator of the Emergency Service (Hospital Provincial General Docente / Riobamba / Ecuador); zullyro@hotmail.com;
3 Resident of the Emergency Service (Hospital Provincial General Docente / Riobamba / Ecuador); aldazl.4amdc.espoch@gmail.com;
4 Resident of the Intensive Care Unit (Hospital Provincial General Docente / Riobamba / Ecuador); katerin_fernanda21@hotmail.com;
5 Resident of the Emergency Service (Hospital Provincial General Docente / Riobamba / Ecuador); marcoalmache26@gmail.com;
* Correspondence: med.carlos.andres@gmail.com; Tel.: +593984109505
ABSTRACT
Bacterial sepsis is one of the most frequent pathologies treated in an intensive care unit. It represents a significant cause of morbidity and mortality at the hospital level, even more so if resistance to antibacterials used as first-line treatment is present. The present study aims to determine the prevalence of Broad-Spectrum Antibiotic Resistance in adult patients over 18 years of age in the Intensive Care Unit of the Hospital Provincial General Docente of Riobamba, Ecuador, in 2023. This is an original, observational, cross-sectional study. The main results are the prevalence of Broad-Spectrum Antibiotic Resistance of 21.9% (95% CI 6.73%-37.02%) and the prevalence of bacterial sepsis of 16% (95% CI 12.2%-19.7%). It is concluded that the prevalence of bacterial sepsis and resistance to broad-spectrum antibacterials is high in the Intensive Care Unit, where the bacteria found most frequently and confer the highest percentage of resistance to septic patients are K. pneumoniae, E. coli and P. aeruginosa.
Keywords: Drug Resistance, Microbial; sepsis; shock, septic
INTRODUCTION
Sepsis corresponds to a clinical syndrome resulting from a deregulated response to changes in physiological, biological, and biochemical effects caused by an infection, which, in addition to an inflammatory response, can produce organ dysfunction, septic shock, and death1,2 . The incidence of sepsis is 31 million people, with a mortality of 6 million per year worldwide, and in Ecuador, a prevalence of 15.1% with a mortality of 47.5%3,4 . The diagnosis of sepsis is given by the presence of an infection, which produces bacteremia, and signs of organ failure are represented by a score greater than or equal to 2 points on the Sequential Organ Failure Assessment (SOFA)5 . There are rapid identification instruments such as the Quick Sequential Organ Failure Assessment (qSOFA) score, the National Early Warning Score (NEWS) score, and the Targeted Realtime Early Warning System (TREWS)2,6 .
Sepsis must be differentiated from Systemic Inflammatory Response Syndrome (SIRS) and Multiple Organ Dysfunction Syndrome (MODS) since, in these two instances, the infectious process may or may not be present, which reduces its specificity, with the particularity that the MODS is a final consequence of septic shock before the patient's death7 .
Cultures are the primary tool to identify the causal agent; however, in half of cases, sepsis presents a negative culture, and the pathogen is not identified8 . Data show bacteria as the predominant pathogens in positive cultures9 . Gram positives are more frequent, among the most common Staphylococcus spp, Streptococcus spp, and Enterococcus spp; on the gram negatives, the most prominent representative is enterobacteria2,10–12 . For this reason, biomarkers have been investigated that help both the early identification of sepsis and its differentiation from SIRS more quickly than cultures13 . Among the biomarkers with the best evidence, we have Procalcitonin (PCT), with a cut-off point of 2ng/mL, and its sensitivity and specificity are more significant than 90%14,15 . The Polymerase chain reaction (PCR) is also helpful as a screening reagent in the acute phase but is elevated in infectious and inflammatory processes; interleukin 6 and 8 (IL6 and IL8) discriminate sepsis from a SIRS used mainly in the pediatric population, and mid regional proadrenomedullin (MRproADM) is superior to PCT in predict mortality in mid and a long term and discriminates between bacterial and viral15 .
Septic patients in an Intensive Care Unit (ICU) are treated with antibiotic therapy regimens that are modified due to the increasing presence of Broad-Spectrum Antibiotic Resistance (BSAR)16 . Antimicrobial resistance generates 700,00 deaths per year; it is linked to an inherent process of microorganisms due to adaptation mechanisms or the inappropriate handling of antibiotics intra and extra-hospital17–19 . We have Broad-Spectrum Antibiotics (BSA) such as carbapenems, cephalosporins, monobactams, and glycopeptides, among others, where the resistance continues to be a growing problem20 .
There are two types of resistance, intrinsic or acquired; the first is inherent to an antimicrobial that is shown by all or almost all members of a species, which makes susceptibility tests unnecessary; a clear example is Klebsiella pneumoniae because it has intrinsic resistance to ampicillin; acquired resistance is the development of resistance to an antimicrobial to which members of the wild-type bacterial population are susceptible, as a result of genetic mutations, horizontal gene transfer through plasmids, integrons, transposons or transformation, or through of a combination of these21–23 . Acquired resistance mechanisms such as antibiotic efflux or expulsion pumps may occur, modification or inactivation of the antibiotic employing hydrolytic enzymes called beta-lactamases that inactivate the antibiotic by hydrolyzing the beta-lactam ring of the molecule24 . The four classes of beta-lactamases are penicillinases, whose substrates correspond to carbapenems; cephalosporinases, cephamycinases and oxacillinases21 . There is global concern about resistance, mainly to Gram-negative bacteria such as E. coli, Klebsiella pneumoniae, Pseudomonas, and Acinetobacter, to counteract this process, new generations of BSA have been incorporated25,26 . Resistance due to ribosomal modification occurs mainly to macrolides (S. pneumoniae and S. pyogenes)24 . Another mechanism is blockingntibiotic entry by changes in the cell membrane, generally gram-negative, and also through biofilms; these bacteria that form the biofilm are protected against dehydration, ultraviolet light, antibiotic and phagocytosis18 .
Current data reveal that both in developing countries and in high-income countries, there is a large amount of resistance to antibacterials, the bacteria that present the most resistance are E. coli, and K pneumoniae, even more so ir the present beta-lactamases of extended spectrum (ESMLs) or K. pneumoniae carbapenemase (KPC)27 . S. aureus and S. pneumoniae are also found, followed by Salmonella spp, and Micobacteria27–30 . Multidrug-resistance (MDR) gram-negative bacilli are one of the main concerns in the health field for causing nosocomial and community infections, particularly NDM-1 Enterobacteriaceae (New Delhi Metallo-beta-lactamase), as well as infection by Clostridium difficile and Pseudomona aeruginosa that drive the search and creation of new classes of antimicrobials with a broader spectrum of action31–35 .
With this introduction, we hypothesize that there is a high prevalence of BSAR used for first-line treatment in adult patients over 18 years of age with a diagnosis of sepsis in the ICU of a public Hospital in Ecuador.
Our general objective is to determine the prevalence of Broad-Spectrum Antibiotic Resistance in adult patients over 18 years of age with a diagnostic of bacterial sepsis in the Intensive Care Unit of the Hospital Provincial General Docente, Riobamba, Ecuador, in 2023. The specific objectives are to establish the prevalence and epidemiological profile of bacterial sepsis in patients over 18 years of age in the ICU of the Hospital Provincial General Docente de Riobamba in 2023, to describe the medical service and the most frequent focus in which antimicrobial resistance occurs, to analyze the relationship between the culture result, and PCT levels with the presence of antimicrobial resistance and to determine the bacteria with the most antimicrobial resistance.
MATERIAL AND METHODS
We present an original observational work corresponding to a cross-sectional study. The information was investigated objectively by a general practitioner specializing in research in Health Sciences, an expert doctor in emergency medicine, and resident doctors of the ICU and emergency department.
In the first instance, the anonymized database provided by HPGDR statistics personnel was reviewed, obtaining the variables to be studied. With a population of 10,840 patients representing total hospital discharges from January to December 2023, inclusion criteria were applied: the presence of sepsis or septic shock either as a main, secondary, or tertiary diagnosis, from the ICU area over 18 years of age, whether from internal medicine, gynecology, and surgery. Exclusion criteria include sepsis or septic shock of viral, fungal, or parasitic origin and those that have not been treated with broad-spectrum antibiotics. 10,465 patients are excluded because they are under 18 years of age and were not hospitalized in the ICU. We obtain a sample of 375 patients. With this sample and applying inclusion and exclusion criteria, we carry out the epidemiological profile of sepsis in the ICU using univariate analysis. The data were collected in Excel, and the analysis was carried out using the SPSS27 statistical package.
Subsequently, the numerator of the calculation of the prevalence of bacterial sepsis is taken as the basis to obtain a new sample guided by the Granmo calculator to determine the epidemiological profile of BSAR, which is the main objective of our study. As a result, an ideal sample of 34 is estimated with 90% confidence, precision of +/- 10 percentage units, a predictable population percentage of 50%, and replacements of 10%. The medical records were reviewed from this ideal sample, and a sample of 32 patients was obtained through simple random sampling.
The statistical staff provided anonymized data with the following variables: diagnosis of sepsis or septic shock, septic focus, culture performed, type of culture, bacteria isolated, initial treatment with BSA, the spectrum of resistance or sensitivity by antibiogram, level of procalcitonin, discharge, comorbidities if rotation antibiotic was necessary and service of origin. Confounding variables: age and sex.
To minimize selection bias, the entire process of obtaining the sample and variables was carried out by the Hospital's statistics staff, which is available for review through authorization so that it can be verified. Strategies to minimize information and measurement bias were not addressed. The first instance database was created in Excel, it was later imported into the SPSS 27 statistical package to carry out the univariate and bivariate analysis, performing statistical tests such as Fisher's exact test, Levene's test, and non-parametric Mann-Whitney U test. The STROBE recommendations were followed for the publication of the results of observational studies.
The Hospital Provincial General Docente de Riobamba (HPGDR) does not have an Ethics Committee for Research (ECR), which is why an institutional review board was held with members of the Health Care Ethics Committee and Hospital authorities to evaluate the relevance and bioethical considerations of the study. After the delivery of the confidentiality commitment by the researchers, covering the ethical concerns and laws for the Protection of patient data expressed in the Declaration of Helsinki of the World Medical Association (WMA), the recommendations on the Protection of participants in the research of the International Committee of Medical Journal Editors (ICMJE), the International Ethical Guidelines for Epidemiological Studies of the Council for International Organizations of Medical Sciences (CIOMS), and for Ecuador, the Organic Health Law of 2006 and the Organic Data Protection Law Personal data from 2021, authorization and general informed consent to obtain anonymized data from medical records were provided by the medical care director of the HPGDR, it was considered an exempt study.
RESULTS
Epidemiological profile of sepsis
The population corresponds to the total number of HPGDR discharges in the year 2023 (n=10,840); 10,465 people are under 18 years of age and were not hospitalized in the ICU; we obtain as a result a sample (n=375) that corresponds to the denominator of the calculation of the prevalence of sepsis. The inclusion (n=62) and exclusion (n=2) criteria are applied, resulting in the numbering for the calculation of the prevalence of sepsis (n=60). The prevalence of bacterial sepsis in patients over 18 years of age (60/375*100) is 16% (95% CI 12.2%-19.7%) in the HPGDR ICU in 2023, 65% are women (n=39), and 35% are men (n=21).
Septic foci are represented in Figure 1. Among the 22 patients with septic urinary focus, 12 were obstetric patients; added to the 6 patients with pure obstetric focus we obtain a result that represents 30% (n=18) of which 33.3% (n=6) due to abortion incomplete or septic and 11.1% had preeclampsia (n=2). For patients with sepsis of abdominal focus, 25% (n=5) were due to peritonitis due to perforated appendicitis, 10% (n=2) due to intestinal obstruction and 5% (n=1) due to surgical site infection.
Only one patient, representing 1.6% of the total number of patients with sepsis, progressed to septic shock.

Figure 1. Distribution of Septic Foci
The comorbidities they presented were Diabetes mellitus 2 11.6% (n=7), acute and chronic kidney disease 6.6% (n=4), pancreatitis 3.3% (n=2), other comorbidities they presented (n=1 per each pathology) were colon cancer, choledocholithiasis, alcoholic hepatitis, cholelithiasis, polycystic ovary, high blood pressure, which together represent 10% and patients without comorbidity 68.5% (n=41).
For hospitalization days, we have an average of 8 days. 66.6% (n=40) belong to Clinic/ICU with an average of 8 days, 18.3% (n=11) represent Gynecology/ICU patients, with an average of 8 days, and for Surgery/ICU with 15% (n=9) average 10 days of hospitalization.
Epidemiological profile of Broad-Spectrum Antibiotic Resistance
To establish that a patient has BSRA, the result of the culture with an antibiogram was considered so much that it had to have a positive outcome that shows the bacteria causing sepsis and that the bacteria is resistant to at least one broad-spectrum antibiotic. In patients with a negative culture with clinical evidence of bacterial infection, it was established that a broad-spectrum antibiotic should have been administered. It would have been necessary to rotate antibiotics to achieve clinical improvement to be considered a patient with BSRA. Therefore, for the sample (n=32) from which we analyzed the epidemiological profile of BSAR, we obtained the following data: 40.6% are men (n=13) and 59.5% are women (n=19). We determined that 78.13% (n=25) do not present BSAR, and 21.9% (n=7) patients present BSAR, as a result, the prevalence of BSAR in patients with bacterial sepsis older than 18 years of the HPGDR ICU in the year 2023 is 21.9% (95% CI 6.73%-37.02%).
The average age among patients with BSAR and patients without BSAR show no differences, with mean age=51 and mean age=50, respectively. There were no patients from surgery with BSAR (n=0); however, the highest percentage of patients with resistance was from the internal medicine service 71% (n=5) followed by gynecology with 28% (n=2). In the case of patients without BSAR, the highest percentage was in internal medicine 56% (n=14), followed by surgery 24% (n=6) and gynecology 20% (n=5).
We obtained an average number of days of hospitalization of 5 days for patients without BSAR and 7 days for those who did not present BSAR in the ICU.
Regarding the diagnosis, 50% (n=16) of the patients had sepsis without evolution to septic shock, of which 37.5% presented BSAR. The remaining 50% had a diagnosis of sepsis that progressed to septic shock, of which 6.25% (n=1) had BSRA.
The proportions of septic foci of the patients with BSAR are described below in Table 1.
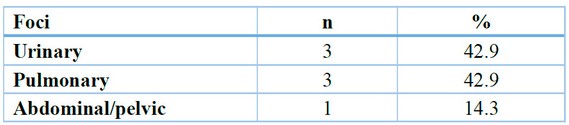
Table 1. Septic foci of the patients with BSAR.
The results obtained from analyzing the cultures in sepsis and septic shock and the organisms identified are shown in Table 2.
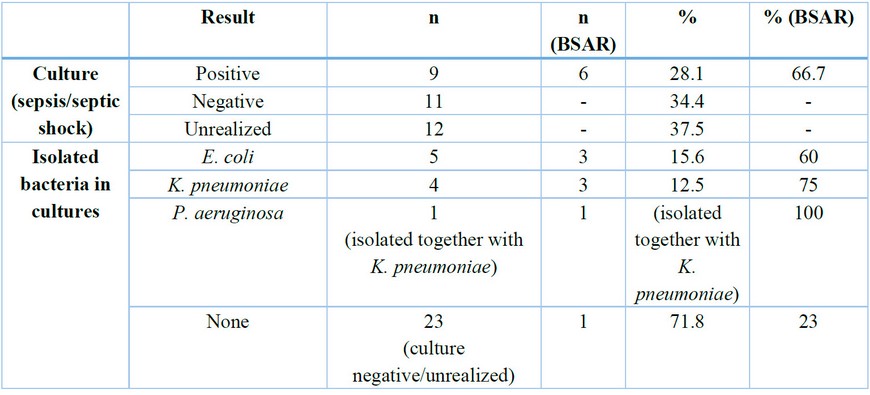
Table 2. Univariate analysis of the results of cultures and isolated bacteria. 2023
100% of patients were treated with broad-spectrum antibiotics as the first line of treatment. In the univariate analysis, no mean differences were shown (mean=2) for patients according to the number of comorbidities, but a difference in averages for the PCT value where a mean of 10.09ng/ml is obtained in patients without BSAR, and patients with BSAR (mean = 6.47ng/ml).
Cultures and antibiograms show greater resistance in bacteria such as K. pneumoniae ESBLs and KPC and E. coli ESBLs.
Table 3 represents the cross-tabulation for the variable's presence of BSAR versus the culture result.

Table 3. Cross tabulation for Presence of BSAR versus Culture result.
We can see in Table 4 how the relationship is quantified using Fisher's exact test between the dependent variable, the presence of BSAR, and the independent variable, the culture result, which shows a statistically significant relationship (p<0.001) between the culture result and BSAR.

Table 4. Fisher's exact test presence of BSAR versus culture result.
We have a continuous quantitative variable corresponding to the PCT whose mean is 9.43 (95% CI 3.34-15.51). To determine if there is a relationship between the dependent variable PTC and the independent variable presence of BSAR, Table 5 shows the equality of variances using the Levene test. Table 6 shows the analysis using the non-parametric Mann-Whitney U test.

Table 5. Levene test for PTC and presence of BSAR.

Table 6. Mann-Whitney U test for PTC and presence of BSAR.
The Levene Test provides us with a level of Significance greater than 0.05, so we establish equality of variances; therefore, the Mann-Whitney U Test with 95% confidence establishes that the levels of PTC do not differ depending on whether or not they present BSAR (p=0.305); as a result, there is no statistically significant relationship.
DISCUSSION
The evidence suggests a percentage growth of 2.1% to 8.7% of patients diagnosed with sepsis at a general level36 . There is not much evidence of the approximate percentage for an intensive care unit, for which this study provides essential information by showing a prevalence of bacterial sepsis of 16%, which is within the actual population value calculated and represents a necessary part of the reality in Ecuadorian public health.
According to the results, the highest percentage of people who present sepsis concerning sex are women, corroborated by the fact that the most frequent septic focus is the urinary tract. Current evidence supports these results since the urinary focus is the most frequent t37 . In our study, the abdominal focus represents only a tiny percentage of the difference concerning the urinary focus. Studies carried out in hospital settings show that abdominal focus is widespread since it derives from surgeries due to complications of acute processes such as appendiceal perforations, leading to peritonitis or Fournier gangrene 38 .
The Control Strategy Against Antibiotic Resistance in Argentina mentions K. pneumoniae and E. colis, the main multidrug-resistant agents 39 . Likewise, in this study, they are the most prevalent along with P. aeruginosa, showing resistance mainly to fourth-generation cephalosporins, carbapenems, aminoglycosides and monobactams. Although this 21.9% prevalence of BSAR does not appear to be worrying, it is worth clarifying that cultures are not always available due to hospital administrative issues, lack of patient resources, or half of the cultures do not identify the etiological agent, considered a negative culture. But when analyzing the data, we realize that when the etiological bacterial agent is identified, 66% present BSAR, which mostly come from the Internal Medicine service, a fact that is corroborated by obtaining a value of Exact Test Fisher significant (p<0.001) to represent the relationship between performing a culture and the presence of BSAR. We can hypothesize that with a larger sample size and a greater number of positive cultures, the value of the prevalence of BSAR would increase considerably, but more research is necessary where a more significant number of cultures are to be analyzed.
PCT is a biomarker used to early detect an infectious process that helps differentiate from SIRS14 . This biomarker is not considered as a possible factor predictor that the septic process presents some type of resistance to the antibiotics used. Consequently, when performing our analysis with the non-parametric Mann-Whitney U model, we can show that we do not obtain a significant value (p>0.05), therefore there is not enough evidence to establish a relationship between the levels of PCT and the appearance or not of BSAR.
This study represents the epidemiological reality of a public Ecuadorian hospital. Being a cross-sectional observational study, it is essential to clarify that there are biases inherent to its design. However, it is the guideline to continue with research and studies of greater scientific power on a threatening reality such as resistance to antibiotics, which are our primary weapon to combat potentially fatal infections.
Strengths and weaknesses
The main strength of our study is that we worked with the entire population to determine the prevalence of bacterial sepsis because the 375 patients represent the total number of patients treated in the intensive care unit in 2023. Although the prevalence of sepsis is not our main objective, our results can be generalized to the population. We intended to work with the entire population with bacterial sepsis (n = 60) to determine the prevalence of BSAR; however, 60 physical clinical histories were not found to review variables by the statistics staff. For this reason, we were forced to perform a sample calculation from those 60 histories. This represents a weakness of the study, as it is a small sample, there is sample bias, and external validity is lost. More studies with a larger sample are necessary for the results to be generalizable to the population.
The Hospital does not keep a good record of clinical histories, which generates data loss. Lost data generated measurement bias, and it was impossible to use regression models to establish relationships with more factors.
As it is a cross-sectional study, we only represent the reality of a specific moment; however, this type of study reflects data that is susceptible to future research with greater rigor and longitudinal design to be able to evaluate changes and impacts of interventions.
We urge the scientific community to investigate and include more intensive care units and to be able to establish results that cover multicenter populations. Our study has an adequate impact on the reality of our Hospital because it provides us with alert data to strengthen medical action and is susceptible to further research.
CONCLUSIONS
Broad-Spectrum Antibacterial Resistance (BSAR) prevalence in adult patients with bacterial sepsis treated in the HPGDR ICU in 2023 was 21.9%. The overall prevalence of bacterial sepsis in this patient population was 16%, with K. pneumoniae, E. coli, and P. aeruginosa identified as the most common causative bacteria. The primary sources of infection were urinary and abdominal, while the main sites of resistance were urinary and pulmonary. Notably, the internal medicine service exhibited the highest rate of resistance.
The study established a correlation between positive culture results and the presence of antimicrobial resistance. However, no association was found between PCT levels and BSAR. The bacteria demonstrating the most significant resistance were ESBL-positive K. pneumoniae and KPC, ESBL-positive E. coli, and P. aeruginosa. These findings underscore the pressing need for continued surveillance and targeted interventions to combat the growing threat of antimicrobial resistance in critical care settings.
Recommendations
In future research, the type of antibiotics and their time of use quantitatively, along with their clinical response, will be analyzed using longitudinal design studies.
Clinical trials or cohort studies should be conducted to measure the effectiveness of interventions by comparing patients from second-level hospitals with third-level ICU patients from specialized hospitals.
Author Contributions: Conceptualization: Md. M.Sc. Carlos Andrés Yépez Salgado; Dr. Zully Mayra Romero Orellana. Data curation, Formal analysis, Methodology, Software, Validation, Visualization and Writing – review and editing: Md. M.Sc. Carlos Andrés Yépez Salgado. Acquisition of funds: project self-financed by the authors. Research: Md. M.Sc. Carlos Andrés Yépez Salgado; Dr. Zully Mayra Romero Orellana; Md. Marco Almache; Md. Katerin Trujillo; Md. Lizeth Aldaz. Project administration: Dr. Zully Mayra Romero Orellana; Md. Katerin Trujillo; Md. Lizeth Aldaz. Resources: Md. Marco Almache; Md. Katerin Trujillo; Md. Lizeth Aldaz. Supervision: Dr. Zully Mayra Romero Orellana; Md. Marco Almache and Writing – original draft: Dr. Zully Mayra Romero Orellana. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding; the APC was funded by the authors.
Institutional Review Board Statement: Ethical review and approval were waived for this study because the methodological nature of the study does not confer ethical conflicts and is considered exempt from evaluation.
Informed Consent Statement: Written general informed consent has been obtained from the medical director of the Hospital.
Data Availability Statement: Anonymized data is available for review in the Hospital's statistics service. The data is delivered upon request to the highest authority of the Hospital.
Acknowledgments: We thank the statistics service, the healthcare ethics committee, and the authorities for supporting the study.
Conflicts of Interest: The authors declare no conflict of interest.
REFERENCES
1. Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Medicine 2017 43:3 [Internet]. 2017 Jan 18 [cited 2024 May 16];43(3):304–77. Available from: https://link.springer.com/article/10.1007/s00134-017-4683-6
2. Sepsis syndromes in adults: Epidemiology, definitions, clinical presentation, diagnosis, and prognosis [Internet]. 2023. Available from: https://www.uptodate.com/contents/sepsis-syndromes-in-adults-epidemiology-definitions-clinical-presentation-diagnosis-and-prognosis/print?search=…1/38www.uptodate.com
3. OPS/OMS | Sepsis: Información General [Internet]. [cited 2024 25 May]. Available from: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=14278:sepsis-general-information&Itemid=72260&lang=es#gsc.tab=0
4. Edison Tarquino Ramos Tituaña1 CECSASHAMCGRJSRGLEBV. Perfil demográfico y epidemiológico de la sepsis en la Unidad de Cuidados Intensivos del Hospital de Especialidades Carlos Andrade Marín [Internet]. Quito; [cited 2024 18 May]. Available from: https://revistahcam.iess.gob.ec/index.php/cambios/article/view/6
5. Gorordo-Delsol LA, Merinos-Sánchez G, Estrada-Escobar RA, Medveczky-Ordoñez NI, Amezcua-Gutiérrez MA, Morales-Segura MA, et al. Sepsis and septic shock in emergency departments of mexico: A multicenter point-prevalence study. Gac Med Mex. 2020;156(6):495–501.
6. Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA - Journal of the American Medical Association. 2016 Feb 23;315(8):762–74.
7. Evaluation and management of suspected sepsis and septic shock in adults [Internet]. 2023. Available from: www.uptodate.com
8. Seetharaman S, Wilson C, Landrum M, Qasba S, Katz M, Ladikos N, et al. Does Use of Electronic Alerts for Systemic Inflammatory Response Syndrome (SIRS) to Identify Patients With Sepsis Improve Mortality? American Journal of Medicine [Internet]. 2019 Jul 1 [cited 2024 May 17];132(7):862–8. Available from: http://www.amjmed.com/article/S0002934319301433/fulltext
9. Uslan DZ, Crane SJ, Steckelberg JM, Cockerill III FR, St Sauver JL, Wilson WR, et al. Age-and Sex-Associated Trends in Bloodstream Infection A Population-Based Study in Olmsted County, Minnesota [Internet]. Available from: https://jamanetwork.com/
10. Ackerman MH, Ahrens T, Kelly J, Pontillo A. Sepsis. Crit Care Nurs Clin North Am. 2021 Dec 1;33(4):407–18.
11. Angus DC, van der Poll T. Severe Sepsis and Septic Shock. New England Journal of Medicine [Internet]. 2013 Aug 29;369(9):840–51. Available from: http://www.nejm.org/doi/10.1056/NEJMra1208623
12. Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score - Development, utility and challenges of accurate assessment in clinical trials. Vol. 23, Critical Care. BioMed Central Ltd.; 2019.
13. Faix JD. Biomarkers of sepsis. Vol. 50, Critical Reviews in Clinical Laboratory Sciences. 2013. p. 23–36.
14. Cercenado E, Rafael M, Moreno C, Carlos J, Díaz R, Carlos Rodríguez J, et al. Diagnóstico microbiológico de la bacteriemia y la fungemia: hemocultivos y métodos moleculares [Internet]. Available from: www.seimc.org
15. Purcarea A, Sovaila S. Sepsis, a 2020 review for the internist. Rom J Intern Med. 2020 Sep 1;58(3):129–37.
16. Chen Q, Li R, Lin CC, Lai C, Chen D, Qu H, et al. Transferability and interpretability of the sepsis prediction models in the intensive care unit. BMC Med Inform Decis Mak [Internet]. 2022 1 December [cited 2024 16 May];22(1). Available from: https://pubmed.ncbi.nlm.nih.gov/36581881/
17. Pierce VM. Overview of antibacterial susceptibility testing [Internet]. 2023. Available from: https://www.uptodate.com/contents/overview-of-antibacterial-susceptibility-testing/print?search=resistenciaantimicrobiana&source=search_result&se…1/32www.uptodate.com
18. Tarín-Pelló A, Suay-García B, Pérez-Gracia MT. Antibiotic resistant bacteria: current situation and treatment options to accelerate the development of a new antimicrobial arsenal. Expert Rev Anti Infect Ther [Internet]. 2022 [cited 2024 May 18];20(8):1095–108. Available from: https://pubmed.ncbi.nlm.nih.gov/35576494/
19. McAdams D, Waldetoft KW, Tedijanto C, Lipsitch M, Brown SP. Resistance diagnostics as a public health tool to combat antibiotic resistance: a modelbased evaluation. PLoS Biol. 2019 May 1;17(5).
20. Martín-Aragón S. ÁMBITO FARMACÉUTICO FARMACOTERAPIA ANTIBIÓTICOS DE ÚLTIMA GENERACIÓN REVISIÓN. Vol. 30.
21. Tamma PD, Doi Y, Bonomo RA, Johnson JK, Simner PJ. A Primer on AmpC β-Lactamases: Necessary Knowledge for an Increasingly Multidrug-resistant World. Clin Infect Dis [Internet]. 2019 Sep 27 [cited 2024 May 17];69(8):1446–55. Available from: https://pubmed.ncbi.nlm.nih.gov/30838380/
22. Wernli D, Søgaard Jørgensen P, Parmley EJ, Majowicz SE, Lambraki I, Carson CA, et al. Scope and applicability of social-ecological resilience to antimicrobial resistance. Lancet Planet Health [Internet]. 2023 Jul 1 [cited 2024 May 17];7(7):e630–7. Available from: https://pubmed.ncbi.nlm.nih.gov/37438004/
23. Livermore DM. Bacterial resistance: origins, epidemiology, and impact. Clin Infect Dis [Internet]. 2003 15 January [cited 2024 17 May];36(Suppl 1). Available from: https://pubmed.ncbi.nlm.nih.gov/12516026/
24. Pouch SM, Ison MG. Deceased donors with multidrug-resistant organisms: implications and future directions. Curr Opin Organ Transplant [Internet]. 2022 Aug 1 [cited 2024 May 17];27(4):250–6. Available from: https://pubmed.ncbi.nlm.nih.gov/36354250/
25. Yahav D, Giske CG, Gramatniece A, Abodakpi H, Tam VH, Leibovici L. New β-lactam–β-lactamase inhibitor combinations. Clin Microbiol Rev. 2021 1 January;34(1):1–61.
26. Astocondor-Salazar L. Betalactamasas: la evolución del problema. Revista Peruana de Investigación en Salud. 2018 Dec 31;2(2):42–9.
27. Tooke CL, Hinchliffe P, Bragginton EC, Colenso CK, Hirvonen VHA, Takebayashi Y, et al. β-Lactamases and β-Lactamase Inhibitors in the 21st Century. 2019 [cited 2024 17 May]; Available from: https://doi.org/10.1016/j.jmb.2019.04.002
28. Abdelaal HFM, Chan ED, Young L, Baldwin SL, Coler RN. Mycobacterium abscessus: It's Complex. Microorganisms [Internet]. 2022 1 July [cited 2024 17 May];10(7). Available from: https://pubmed.ncbi.nlm.nih.gov/35889173/
29. Caminero Luna JA, Pérez Mendoza G, Rodríguez de Castro F. Multi-drug resistant tuberculosis, ten years later. Med Clin (Barc) [Internet]. 2021 Apr 23 [cited 2024 May 18];156(8):393–401. Available from: https://pubmed.ncbi.nlm.nih.gov/33531151/
30. Carrillo-Córdova LD, Aguilar-Aizcorbe S, Hernández-Farías MA, Acevedo-García C, Soria-Fernández G, Garduño-Arteaga ML. [Escherichia coli productora de betalactamasas de espectro extendido como agente causal de gangrena de Fournier de origen urogenital asociada a mayor mortalidad]. Cir Cir [Internet]. 2018 Jul 1 [cited 2024 May 18];86(4):327–31. Available from: https://pubmed.ncbi.nlm.nih.gov/30067712/
31. Bose P, Rangnekar A, Desikan P. NDM-beta-lactamase-1: Where do we stand? Vol. 155, Indian Journal of Medical Research. Wolters Kluwer Medknow Publications; 2022. p. 243–52.
32. Ocampo-Ríos AM, Giraldo-Gómez MB LM, Melo-Álvarez MB KL, Obando-Agreda MB AC, Natalia Jiménez-Quiceno J. Variations in the modified Hodge test to detect carbapenemase production in Pseudomonas aeruginosa. Vol. 21, Investigación Medicina & Laboratorio. 2015.
33. Lai CC, Yu WL. Klebsiella pneumoniae Harboring Carbapenemase Genes in Taiwan: Its Evolution over 20 Years, 1998–2019. Vol. 58, International Journal of Antimicrobial Agents. Elsevier B.V.; 2021.
34. Czepiel J, Dróżdż M, Pituch H, Kuijper EJ, Perucki W, Mielimonka A, et al. Clostridium difficile infection: review. European Journal of Clinical Microbiology and Infectious Diseases [Internet]. 2019 Apr 3 [cited 2024 May 18];38(7):1211–21. Available from: https://link.springer.com/article/10.1007/s10096-019-03539-6
35. Lim SC, Knight DR, Riley T V. Clostridium difficile and One Health. Clin Microbiol Infect [Internet]. 2020 Jul 1 [cited 2024 May 18];26(7):857–63. Available from: https://pubmed.ncbi.nlm.nih.gov/31682985/
36. Esposito S, De Simone G, Boccia G, De Caro F, Pagliano P. Sepsis and septic shock: New definitions, new diagnostic and therapeutic approaches. J Glob Antimicrob Resist [Internet]. 2017 1 September [cited 2024 31 May];10:204–12. Available from: https://pubmed.ncbi.nlm.nih.gov/28743646/
37. Doi Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin Infect Dis [Internet]. 2019 Nov 13 [cited 2024 May 18];69(Suppl 7):S565–75. Available from: https://pubmed.ncbi.nlm.nih.gov/31724043/
38. López-Fernández J, García Plaza G, Antón Fernández I. Mediastinal Escherichia coli abscess during Fournier’s gangrene. Med Clin (Barc) [Internet]. 2022 Jan 7 [cited 2024 May 18];158(1):40–1. Available from: https://pubmed.ncbi.nlm.nih.gov/34103167/
39. Lazovski J, Corso A, Pasteran F, Monsalvo M, Frenkel J, Cornistein W, et al. Estrategia de control de la resistencia bacteriana a los antimicrobianos en Argentina. Rev Panam Salud Publica [Internet]. 2017 [cited 2024 31 May];41. Available from: https://pubmed.ncbi.nlm.nih.gov/31391822/
Received: 1 June 2024 / Accepted: 16 August 2024 / Published: 15 September 2024
Citation: Carlos Yepez; Zully Romero; Lizeth Aldaz; Katerin Trujillo ; Marco Almache. Broad-Spectrum Antibiotic Resistance in septic Patients in an Ecuadorian Intensive Care Unit of the Hospital Provincial General Docente of Riobamba. Bionatura Journal 2024; 1 (3) 13. http://dx.doi.org/10.70099/BJ/2024.01.03.13
ISSN. 3020-7886
Additional information Correspondence should be addressed to: med.carlos.andres@gmail.com
Peer review information. Bionatura thanks anonymous reviewer(s) for their contribution to the peer review of this work using https://reviewerlocator.webofscience.com/
All articles published by Bionatura Journal are made freely and permanently accessible online immediately upon publication, without subscription charges or registration barriers.
Publisher's Note: Bionatura Journal stays neutral concerning jurisdictional claims in published maps and institutional affiliations.
Copyright: © 2024 by the authors. They were submitted for possible open-access publication under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).